Case Report
Preservation of Haemostasis with Anti-thrombotic Serotonin Antagonism

Mark IM Noble1* and Angela J Drake-Holland2
1University of Aberdeen, Aberdeen, Scotland
2Robert Gordon University, Aberdeen, Scotland
*Address for Correspondence: Mark IM Noble, University of Aberdeen, Aberdeen, Scotland, Email: [email protected]
Dates: Submitted: 18 August 2017; Approved: 15 September 2017; Published: 18 September 2017
How to cite this article: Noble MIM, Holland AJD. Preservation of Haemostasis with Anti-thrombotic Serotonin Antagonism. J Hematol Clin Res. 2017; 1: 019-025. DOI: 10.29328/journal.jhcr.1001004
Copyright License: © 2017 Noble MIM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Abstract
An enquiry into the lack of attention awarded to serotonin antagonism in the treatment of arterial thrombosis revealed that the mode of action of serotonin and its platelet receptor antagonists was an action upon thrombus growth, and not, as with other anti-platelet drugs upon the initiation of thrombosis. This lack of effect could explain why this approach has been considered not to be effective. However under conditions of arterial stenosis in which there is platelet activation by increased shear stress, and during the growth phase of arterial thrombi, serotonin 5HT2A antagonism has been demonstrated to have great potentcy in dispersing thrombotic obstruction to blood flow. This mode of action, the lack of participation of serotonin in haemostasis, and the absence of serotonin in wounds accounts for the proven lack of effect of effect of pure specific 5HT2A antagonists (i.e., not those with other actions) on operative bleeding and skin bleeding times. This lack of effect on haemostasis solves the dosing problem encountered with other anti-thrombotic drugs, with which drug concentration cannot be controlled with single fixed doses, leading to the association between increased anti-thrombotic efficacy and increased bleeding complications. Thus 5HT2A antagonism appears to be the preferred approach, from the point of view of safety and lack of bleeding risk; this consideration applies particularly to thrombosis therapy in the context of traumatic accidents, surgical operations and invasive procedures such as angioplasty.
Introductıon
The importance of control of intra-arterial thombosis is enhanced if this process proves crucial to the development of atherothrombosis as well as to the terminal stages [1,2]. It is commonly thought that thrombosis and haemostasis are always linked, leading to the concept that anti-thombotic therapy is inevitably associated with excess bleeding, also called ‘bleeding risk’ [3]. It is true that experience with anticoagulants, which inhibit the action of thrombin, either directly or via the coagulation cascade, and with anti- platelet agents, which inhibit the thromboxane, purine or glycoprotein receptors, has confirmed the bleeding risk with these approaches [4]. At the present time, no alternative approach has been accepted, but in the case of anti-thrombotic treatment of arterial thrombosis, in which thrombin antagonism is ineffective [5] an alternative approach is available, namely inhibition of the serotonin receptor [6-10]. This follows the recommendation of [11], that drugs which block events upstream of the final common pathway might be better antiplatelet agents than those that merely inhibit platelet aggregation.
The anti-serotonin approach
Serotonin (5-hydroxytryptamine, 5HT) is present in high concentration in blood platelets. In contrast to the thromboxane, purine or glycoprotein mediators, serotonin does not influence the formation of haemostatic layers, although it is implicated in shear-induced aggregation and thrombus propagation by positive feedback from the large amount of intra-platelet serotonin. It is important to distinguish between the serotonergic receptor subtypes [12]. 5HT1 receptors respond with endothelium dependent nitric oxide mediated vasodilatation; 5HT2 receptors activate platelets and mediate smooth muscle contraction. Thus, in arterial lesions in which vascular smooth muscle is bared of endothelium, vasoconstriction excacerbates arterial occlusion by thrombus; relief of such vasoconstriction by 5HT2A antagonists is a bonus. However, surprisingly to date, serotonin antagonism has not progressed to clinical application in spite of publications confirming the effects of such antagonism, [13].
Platelets are the richest source of serotonin in the body outside the brain. Serotonin is not the only molecule secreted by platelets; the other include ADP, ATP, GDP, pyrophosphate, magnesium and calcium [14]. Platelets acquire serotonin from the plasma by means of the cell membrane serotonin uptake mechanism [15], and store the serotonin in dense granules [14]. Inhibition of this mechanism by serotonin re-uptake inhibitors (SSRIs) causes depletion of platelet serotonin [16].
Serotonin dependence of acute arterial thrombosis and its inhibition by 5HT2A antagonism
Upon platelet activation (especially with high shear) high concentrations of serotonin in the platelets are released from the dense granules [17] and act upon platelet serotonin 5HT2A receptors to activate more platelets, thus constituting a positive feedback mechanism leading to thrombus growth [18]. The serotonin theory [8] supposes that this serotonin mediation is essential for thrombotic occlusion of diseased coronary arteries, owing to the fact that such occlusions are abolished by antagonism of the platelet 5HT2A receptor [9,19] even when the major stimulus of adrenaline is applied [20] and also in the circumstances where thrombolysis has failed to clear a complete thrombotic occlusion [21].
Examination of patients undergoing angiography has showed that a high plasma serotonin level was significantly associated with coronary artery disease in patients younger than 70. In nearly four years of follow up, high serotonin levels were also associated with cardiac events. This association persisted after adjustment for conventional risk factors [22].
Unfortunately, most of the antagonists of the platelet the 5HT2A serotonin receptor have encountered problems. These problems are not due to the receptor blockade, but have precluded their application to human arterial thrombosis. However, Th001 (ArteclereTM) formerly known as ICI170809 [23], or AZ170809, has proved extremely potent as an inhibitor of intracoronary thrombus growth [20]. This drug appeared to be safe in a number of trials of toxicity, which are detailed in an Investigator’s Brochure. Another important aspect of the McAuliffe results [20] and those of [19], is that arterial thrombi spontaneously disperse under the influence of 5HT2A antagonism to clear the artery for full blood flow. We presume that this is due to intrinsic natural thrombolyic agents [24]. The possibiity that the 5HT2A antagonist ICI170809 itself has a lytic effect was disproved by experiments in Aberdeen (unpublished). Indeed clearance of thrombus by thrombolytic drugs such as tPA is followed in dogs by re-occlusion, which 5HT2A antagonism prevents [21]. These results are compatible with the intrinsic anti-thrombolytic effect [24]./p>
A potent reason for pharmaceutical groups to promote 5HT2A antagonism is the involvement of 5HT2A receptors in promoting thrombosis in diabetes [25]. This disease is now reaching epidemic proportions worldwide with cardiovascular complications being the leading reason for morbidity and mortality in diabetes mellitus.
Other 5HT2A receptor antagonists have been available in the past that also showed efficacy in acute arterial thrombosis, e.g., ketanserin [26] ritanserin [9], LU 49938 [27], MDL11,939, and LY53,857 [21], MDL 28,133A [28], DV-7028 [29], AT-1015 [30,31], APD791 [32-34]. The 5HT2A antagonists presently available are Th001 (ArteclereTM), a specific platelet receptor antagonist and nefazodone [35], an antidepressant now taken off the market with non-platelet effects and an unknown effect on thrombosis. At present, sarpogrelate [36] seems to be the only 5HT2 antagonist in clinical application. It is used in a wide variety of cardiovascular diseases associated with thrombosis, but appears not to have been trialed in acute coronary syndromes. Th001 (ArteclereTM) has had considerable exposure in humans, with a clean safety record. We find confusing those studies of drugs with mixed receptor subtype, e.g., SL65.0472 [10].
Why has the serotonin approach not been followed up?
This follows from the different mode of action of serotonin and its antagonists, namely activation by increased shear stress [37], and blockade of positive feedback of serotonin generating thrombus growth. Most reports on the effects of 5HT2A antagonists do not consider shear stress as an activating stimulus, [13]. But, increased shear stress is the very haemodynamic stimulus that occurs in a stenosed artery, and accounts for thrombus formation in both eccentric and concentric coronary artery lesions. Confirmation that 5HT2A receptors play a major role in high-shear rate thrombus formation is provided by [38]. When searching for possible antiplatelet drugs, pharmaceutical groups search for platelet aggregability that is often tested in citrated platelet rich plasma, in which calcium ions have been removed. With this approach, high aggregability is found to thromboxane and ADP, together with high potency of their antagonists, compared to little or no activity using serotonin and its antagonists. They thus incorrectly ignore the role of shear stress within stenoses and the involvement of 5HT2A receptors in that process, and assume that serotonin antagonists are ineffective. This conclusion is made despite the McAuliffe’s 1993 study [20], in which ICI170809 showed about ten times the potency of clopidogrel, the leading P2Y12 purine (ADP) receptor antagonist, in inhibition of growing thrombus in vivo.
A second factor that deterred pharmaceutical groups from the serotonin antagonism approach is that the first 5HT2 antagonist caused multiple problems due to its non-5HT2 properties. One of these was alpha-1 antagonism causing a drop in arterial pressure leading to trial in hypertension! Pure 5HT2 serotonin receptor antagonism has absolutely no role in the treatment of hypertension [39]. The other adverse effect of ketanserin was more serious, that of prolongation of the cardiac action potential and QT interval, causing deaths from arrhythmias. Since that time serotonin antagonists have been rigorously investigated, e.g., Th001 (ArteclereTM), with the result that there is a clear absence of any cardiac electrophysiological changes attributed to serotonin or Th001 (ArteclereTM).
Superiority of the serotonin approach in haemostasis
Those performing research on 5HT2 antagonists since the 1980s when ketanserin became available, have observed that the haemostatic layer of blood cells bound to fibrinogen is unaffected. All the early work with these compounds involved experimental surgery on animals, and it was of note that, unlike similar experiments with other anti-thrombotic drugs, there was no excess bleeding, and no oozing coagulopathy. This makes these drugs particularly attractive to surgeons wanting to protect their patients from arterial thrombosis in the peri-operative period [40]. So, is it possible that, contrary to received opinion, the anti-thrombotic activity of 5HT2A antagonists can be accompanied by an absence of effect on haemostasis. That this can be the case follows from the fact that the anti- thrombotic action only comes into effect during the thrombus growth phase of the occlusive arterial thrombosis process, the lack of participation by serotonin in the haemostatic process and the absence of serotonin in wounds.
Some drugs called 5HT2A receptor antagonists have been claimed to prolong bleeding when cutting off the tails of mice [41], or rats [30,42], both containing veins. These claims need to be confirmed by correct methodologically controlled skin bleeding time measurements in man as performed by [43]. This study carried out at Aberdeen Royal Infirmary by [43], an MHRI approved report in the public domain that is now published, investigated indices of haemostasis in 48 patients with stable arterial disease. This stability enabled the investigators to design a statistically paired, randomised cross- over trial of placebo versus Th001 (ArteclereTM). Lack of effect on haemostasis was confirmed by a series of ultegra and flow cytometry tests. Skin bleeding time showed no significant difference. Another important aspect of this study was that the dosing used for the Th001 (ArteclereTM) arm (10mg bd for 2 weeks) produced a considerably higher plasma drug concentration than that producing complete arterial clearance in the McAuliffe study [20]. This is an important consideration when investigating dosing of other anti-thrombotic drugs.
The dosing problem with anti-thrombotic therapy
The efficacy of drug action is a function of drug concentration according to the classical concentration-effect relationship (Figure 1).
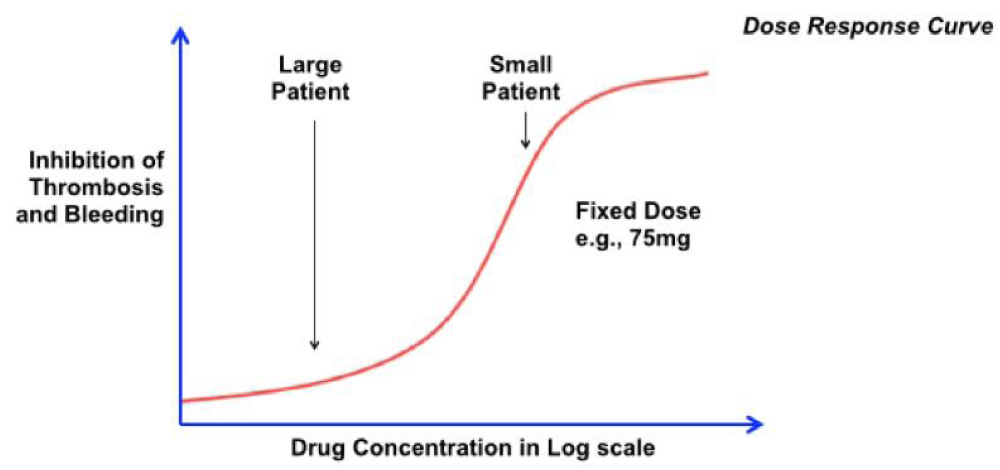
Figure 1: When drugs affect both thrombosis and haemostasis, a single fixed dose regime, e.g., 75mg clopidogrel gives different concentrations for different body masses. A large patient may be inadequately treated whereas a small patient may have bleeding complications.
When drugs affect both thrombosis and haemostasis, a single fixed dose regime, e.g., 75mg clopidogrel gives different concentrations for different body masses. A large patient may be inadequately treated whereas a small patient may have bleeding complications. Only a lucky patient may receive a dose giving the correct concentration, but only by chance (Figure 2). Sensitivity to a given drug concentration varies from patient to patient. A patient with the blue concentration-effect curve in figure 3 will be inadequately treated, whereas one with the green relationship will have high bleeding risk. The ideal solution is to use a pure selective 5HT2A antogonist such as Th001 (ArteclereTM) which only affects thrombosis and not haemostasis; then one can give a high dose (right hand arrow in Figure 3), that is safe for all patient weights and sensitivities.
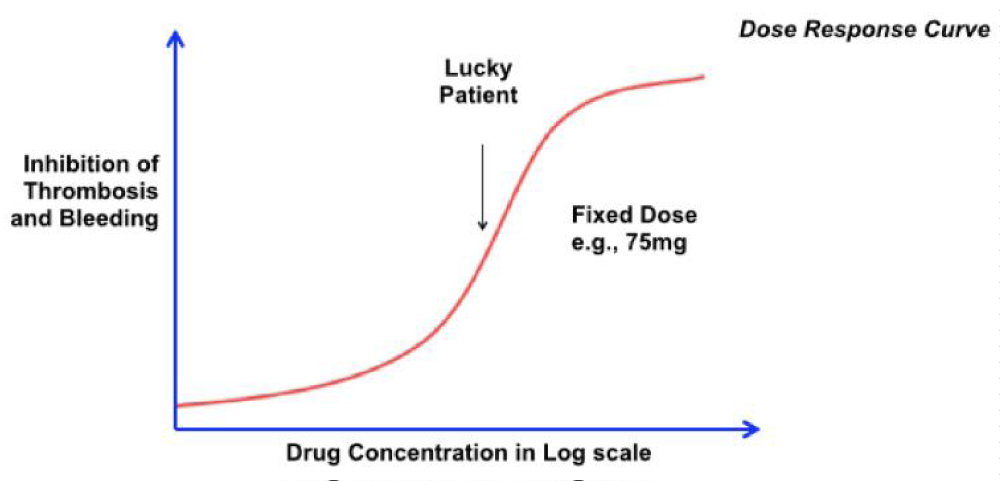
Figure 2: A lucky patient may receive a dose giving the correct concentration, but only by chance.
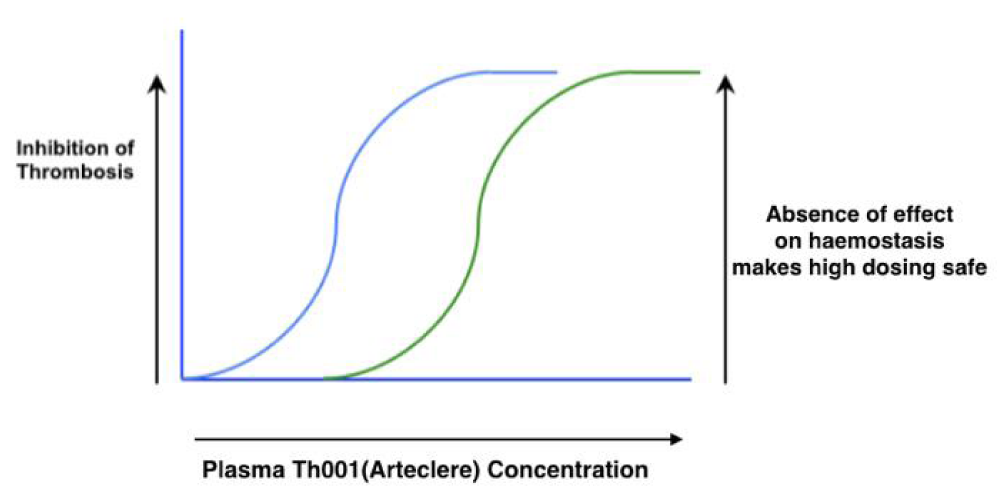
Figure 3: Patients’ sensitivities to a given drug concentration varies. Overdosing with a 5HT2A antagonist with no effect on haemostasis avoids these problems (right hand arrow).
Conclusion
5HT2A antagonism is proposed as the ideal solution to the problem of bleeding associated with treatment of arterial thrombosis. In the development of this approach, it is important to use a pure selective 5HT2A antogonist such as Th001 (ArteclereTM) which only affects thrombosis and not haemostasis. The reason for this conclusion is that thrombosis in arterial stenoses is activated by increased shear stress causing release of serotonin from platelets that then activates more platelets, setting in train the serotonin dependent positive feedback mechanism. This process is blocked by antagonism of the platelet 5HT2A receptor. Because of the absence of effect of 5HT2A antagonism on haemostasis, one can give a high dose that is safe for all patient weights and drug sensitivities. Of the 5HT2A antagonists that have been investigated, Th001 (ArteclereTM) has had a large exposure in human volunteers and patients and has not caused significant adverse effects.
References
- Noble MIM. Thrombosis as a unitary hypothesis of cardiovascular risk. J Cardiovasc Risk. 1995; 2: 177-179. Ref.: https://goo.gl/p8t1XC
- Steinhubi SR, Moliterno DJ. The role of the platelet in the pathogenesis of atherothrombosis. Am J Cardiovasc Drugs. 2005; 5: 399-408. Ref.: https://goo.gl/dpxsc8
- De Meyer SF, Vanhoorelbeke K, Broos K, Salles II, Deckmyn H. Antiplatelet drugs. Br J Haematol. 2008; 142: 515-528. Ref.: https://goo.gl/af7yNg
- Jennings LK. Mechanisms of platelet activation: need for new stratgies to protect against platelet- mediated atherothrombosis. Thromb Haemost. 2009; 102: 248-257. Ref.: https://goo.gl/ogSSLa
- Belcher PR, Drake-Holland AJ, Hynd JW, Noble MIM. Failure of thrombin inhibition to prevent intracoronary thrombosis in the dog. Clin Sci (Lond). 1996; 90: 363-368. Ref.: https://goo.gl/nR7GY7
- Noble MIM, Drake-Holland AJ. The involvement of serotonin in the formation of thrombi at critical coronary artery stenoses in humans. Coronary Artery Disease. 1990; 1: 675-679. Ref.: https://goo.gl/uoVgST
- Noble MIM, Drake-Holland AJ. The possible role of serotonin 5HT2 receptor antagonism in cardioprotection. Neth J Med. 1992; 41: 183-189. Ref.: https://goo.gl/r92Eid
- Noble MIM, Drake-Holland AJ. The role of serotonin 5HT2 receptor antagonism in the control of coronary artery disease. Q J Med. 1994; 87: 11-16. Ref.: https://goo.gl/wbKmLj
- Torr S, Noble MIM, Folts JD. Inhibition of acute platelet thrombosis formation in stenosed canine coronary arteries by the specific serotonin 5HT2 receptor antagonist ritanserin. Cardiovasc Res. 1990; 24: 465-470. Ref.: https://goo.gl/KtDHLQ
- Moerland M, Kemme M, Dijkmans A, Bergougnan L, Burrggraaf J. Modulation of vasoactivity and platelet aggregation by selective 5-HT receptor antagonism in humans. J Cardiovasc Pharmacol. 2011; 58: 575-580. Ref.: https://goo.gl/SWQNk3
- Goto S. Understanding the mechanism and prevention of arterial occlusive thrombus formation by anti-platelet agents. Curr Med Chem cardiovasc Hematol Agents. 2004; 2: 149-156. Ref.: https://goo.gl/Y1DNq4
- Van Nueten JM, Leysen JE, de Clerk F, Vanhoutte PM. Serotonergic receptor subtypes and vascular reactivity. J Cardiovasc Pharmacol. 1984; 6: 564-574. Ref.: https://goo.gl/L7ZWWZ
- Hara H, Osakabe M, Kitajima A, Tamao Y, Kikumoto R. MCI-9042, a new antiplatelet agent is a selective s2-serotonergic receptor antagonist. Thromb Haemost. 1991; 65: 415-420. Ref.: https://goo.gl/d2UEfd
- Golebiewska EM, Poole AW. Platelet secretion: From haemostasis to wound healing and beyond. Blood Rev. 2015; 29: 153-162. Ref.: https://goo.gl/LpvjB1
- Brenner B, Harney JT, Ahmed BA, Jeffus BC, Unal R, et al. Plasma serotonin levels and the platelet transporter. J Neurochem. 2007; 102: 206-215. Ref.: https://goo.gl/UErvuT
- Menys VC, Smith CCT, Lewins P, Farmer RDT, Noble MIM. Platelet 5-hydroxytryptamine is decreased in a preliminary group of depressed patients receiving the 5-hydroxytryptamine re-uptake inhibiting drug fluoxetine. Clin Sci (Lond). 1996; 91: 87-92. Ref.: https://goo.gl/WMAFSu
- Cerrito F, Lazzaro MP, Gaudio E. Arminio P, Aloisi G. 5HT2-receptors and serotonin release: their role in human platelet aggregation. Life Sci. 1993; 53: 209-215. Ref.: https://goo.gl/igVXKw
- De Clerck F. The role of serotonin in thrombogenesis. Clin Physiol Biochem. 1990; 3: 40-49. Ref.: https://goo.gl/F4fTL4
- Belcher, PR, Drake-Holland AJ, Hynd J, Noble MIM. Dispersion of coronary artery thrombi by antagonism of platelet serotonin receptor in the dog. Cardiovasc Res. 1992; 26: 292-296. Ref.: https://goo.gl/no2Kz5
- McAuliffe SJG, Snow HM, Cox B, Smith CTT, Noble MIM. Interaction between the effect of 5-hydroxytryptamine and adrenaline on the growth of platelet thrombi in the coronary artery of the anaesthetised dog. Br J Pharmacol. 1993; 109: 405-410. Ref.: https://goo.gl/QqDdHK
- Belcher PR, Drake-Holland AJ, Noble MIM. Antagonism of the platelet 5HT2 receptor in the presence of thrombolysis. Int J Cardiol. 1994; 43: 11-20. Ref.: https://goo.gl/gZmge7
- Vikenes K, Farstad M, Nordrehaug JE. Serotonin is associated with coronary artery disease and cardiac events. Circulation. 1999; 100: 483-489. Ref.: https://goo.gl/7zZC32
- Millson DS, Jessop CL, Swaisland A, Haworth S, Rushton A, et al. The effect of a selective 5HT2 receptor antagonist (ICI 170,809) on platelet aggregation and puplillary responses in healthy volunteers. Br J Clin Pharmacol. 1992; 33: 281-288. Ref.: https://goo.gl/59y1WZ
- Vandeplassche G, Hermans C, Van Dael L, Wouters l, De Clerke F. Interplay between platelet- derived 5HT and arachidonic acid metabolites limits the thrombolytic efficacy of streptokinase against canine plateler-rich coronary thrombosis. J Cardiovasc Pharmacol. 1993; 21: 56-69. Ref.:
https://goo.gl/Ub8Nsw - Yamada K, Niki H, Nagai H, Nishikawa M, Nakagawa H. Serotonin potentiates high-glucose- induced endothelial injury: the role of serotonin and 5-HT2A recptors in promoting thrombosis in diabetes. J Pharmacol Sci. 2012; 119: 243-250. Ref.: https://goo.gl/sWYXP4
- Ashton JH et al. Serotonin as a mediator of cyclical flow variation in stenosed canine coronary arteries. Circulation. 1986; 73: 572-578. Ref.: https://goo.gl/FSZqUp
- Kirchengast M, Rubsamen K & Lehmann HD. Inhibition by the combined Ca2+ and 5-HT2 receptor antagonist nexopamil (LU 49938) of intracoronary thrombus formation in a canine model of arterial stenosis and intimal damage. J Cardiovasc Pharmacol. 1993; 22: 687-694. Ref.:
https://goo.gl/GS6naX - Hsieh CP, Sakai K, Bruns GC, Dage RC. Effects of MDL 28,133A, a 5-HT2 receptor antagonist, on platelet aggregation and coronary thrombosis in dogs. J Cardiovasc Pharmacol. 1994; 24: 761-772. Ref.: https://goo.gl/otkqNv
- Pawlak D, Pawlak K, Chabielska E, Malyszko J, Takada A, et al. A potent 5HT receptor (5-HT2A) antagonist, DV-7028, delays arterial thombosis development in rats. Thromb Res. 1998; 90: 259-270. Ref.: https://goo.gl/YjmaUJ
- Kihara H, Koganei H, Hirose K, Yamamoto H, Yoshimoto R. Antithrombotic activity of AT-1015, a potent 5-HT2A recptor antagonist, in rat arterial thrombosis model and its effect on bleeding time. Eur J Pharmacology. 2001; 21:157-162. Ref.: https://goo.gl/beQVVZ
- Rashid M, Watanobe M, Nakazawa M, Nakamura T, Hattori K, et al. Assessment of affinity and dissociation of newly synthesized 5-HT2 antagonist, AT-1015: comparison with other 5-HT2 antagonists. Jpn J Pharmaccol. 2001; 87: 189-194. Ref.: https://goo.gl/vXf67z
- Adams JW et al. APD791, a novel 5HT2A receptor antagonist: pharmacological profile, pharmacokinetics, platelet activity and vascular biology. J Pharmacol Exp Ther. 2009; 331: 96-103. Ref.: https://goo.gl/2QSs3x
- Przyklenk K, Frelinger AL3rd, Linden D, Whittaker P, Li Y, et al. Targeted inhibition of the serotonin 5HT2 receptor improves coronary patency in an in vivo model of recurrent thrombosis. J Thromb Haemost. 2010; 8: 331-340. Ref.: https://goo.gl/4VAofo
- Xiong Y, Teegarden BR, Choi JS, Strah-Pleynet S, Decaire M, et al. Discovery and structure- activity relationship of APD791: a highly selective 5HT2A receptor inverse agonist for the treatment of arterial thrombosis. J Med Chem. 2010; 53: 4412-4421. Ref.: https://goo.gl/uDj4Sh
- Sussman N, Ginsberg DL, Bikoff J. Effects of nefazodone on body weight: a pooled analysis of selective serotonin reuptake inhibitor-and imipramine-controlled trials. J Clin Psychiatry. 2001; 62: 256-260. Ref.: https://goo.gl/1dwes2
- Nagatomo T, Rashid M, Abul Muntasir A, Komiyama T. Functions of 5HT2A receptor and its antagonists in the cardiovasclar system. Pharmacol Ther. 2004; 104: 59-81. Ref.: https://goo.gl/gtj7DR
- Sakariassen KS, Hanson SR, Cadroy Y. Methods and models to evaluate shear-dependent and surface reactivity-dependent antithrombotic efficacy. Thromb Res. 2001; 104: 149-174. Ref.: https://goo.gl/rGTRT1
- Valentin JP, View S, Bertolino F, Faure´P, John G. Differential involvement of serotonin 2A/C and thromboxane A2/prostenoid receptors in high- vs. low-shear rate arterial thrombosis in rabbits. J Pharmacol Exp Ther. 1997; 280: 761-769. Ref.: https://goo.gl/mQpcsf
- Stott DJ, Saniabadi AR, Hosie J, Lowe GDO, Ball SG. The effects of the 5HT2 antagonist ritanserin on blood pressure and serotonin-induced platelet aggregation in patients with untreated essential hypertension. Eur J Clin Pharmacol. 1988; 35: 123-129. Ref.: https://goo.gl/mwFrbY
- Vincentelly A, Jude B, Belisle S. Antithrombotic therapy in cardiac surgery. Can J Anaesth. 2006; 53: 89-102. Ref.: https://goo.gl/CxjDgU
- Lin OA, Karim ZA, Vemana HP, Espinosa EV, Khasawneh FT. The antidepressant 5-HT2A receptor antagonists piztifen and cyproheptadine inhibit serotonin-enhanced platelet function. PLoS One. 2014; 23: 87026. Ref.: https://goo.gl/E8J4zh
- Adams JW, Ramirez J, Ortuno D, Shi Y, Thomsen W, et al. Anti-thrombotic and vascular effects of AR246686, a novel 5-HT2A receptor antagonist. Eur J Pharmacol. 2008; 586: 234-243. Ref.: https://goo.gl/h535k1
- Noble MIM, Ford I, Cameron G, Drake-Holland AJ. The novel anti-thrombotic drug with no bleeding excess. J Cardiol Cardiovasc Therap. 2017.