
More Information
Submitted: May 19, 2021 | Approved: June 03, 2021 | Published: June 04, 2021
How to cite this article: Hasan FMM, Gomes RR. Demographic profile & correlation between retinal exudates and hematological parameters in leukemic patients. J Hematol Clin Res. 2021; 5: 009-014.
DOI: 10.29328/journal.jhcr.1001017
ORCID: orcid.org/0000-0002-2511-7972
Copyright License: © 2021 Hasan FMM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Leukemic retinopathy; Retinal exudates; Thrombocytopenia; Anemia

Demographic profile & correlation between retinal exudates and hematological parameters in leukemic patients
FM Monjur Hasan1 and Richmond Ronald Gomes2*
1Associate Professor, Medicine, Ad-din Sakina Women’s Medical College Hospital, Jashore, Bangladesh
2Associate Professor, Medicine, Ad-din Women’s Medical College Hospital, Dhaka, Bangladesh
*Address for Correspondence: Dr. Richmond Ronald Gomes, Associate Professor, Medicine, Ad-din Women’s Medical College Hospital, Dhaka, Bangladesh, Email: [email protected]
Background: Leukemia is frequently associated with fundoscopic abnormalities. However, no organized effort has been made for analyzing leukemic retinopathy in our country. This study was done to observe the demographic profile and correlation between fundoscopic findings of retinal exudates and hematological parameters in leukemic patients.
Materials and Methods: The study was a hospital-based descriptive cross-sectional study among 50 leukemic patients in Medicine and Oncology departments of Bangladesh Medical College and Hospital (BMCH) from May, 2020 to October, 2020. Fundoscopic examination was done which was reviewed by an ophthalmologist. Collected data was analyzed statistically by using SPSS-17 (Chicago, Illinois).
Results: Among 50 leukemic patients’, the fundal lesion was detected in 32 patients (64%), retinal exudates are rare. Only 3 patients (6%) had exudates while others (29 patients, 58%) have retinal hemorrhages. Exudates did not show any statistically significant relationship with types of leukemia (p value = 0.53). There was no statistically significant association between fundal exudates and high white cell count (p = 0.56) or low hemoglobin level (p = 0.11) or low platelet level (p = 0.11).
Conclusion: This study has identified retinopathy occurring frequently in leukemic patients. Therefore, an adequate attention should be paid at fundoscopic evaluation while treating leukemic patients.
Leukemia is a malignant proliferative disorder of leukopoitic bone marrow stem cells characterized by over-crowding of the bone marrow by immature neoplastic leukocytes and widespread infiltration of organs, tissues and peripheral blood by immature leukocytes [1]. The resultant displacement of normal haemopoitic stem cells from the bone marrow leads to secondary hematologic complications such as erythropenia, thrombocytopenia and leukostasis. Although there is peripheral leukocytosis, the circulating leukocytes are immature and dysfunctional. The secondary hematologic alterations are responsible for tissue ischemia, bleeding diathesis, immunosuppression, and hyperviscosity state which are the cardinal pathological features of leukaemia [2].
Based on cell types, differentiation, morphology, cytogenetic characteristics and immunophenotyping, leukemia is classified into acute and chronic subgroups. Each subgroup further sub-divided into myeloblastic and lymphoblastic variants such as acute lymphoblastic leukemia (ALL), acute myeloblastic leukemia (AML), chronic lymphocytic leukemia (CLL) and chronic myelocytic leukemia (CML) [1-3]. In a study, reports of patients with acute lymphoblastic leukemia presenting with visual symptoms as the initial sign of the disease are rare. However, the ocular changes in acute lymphoblastic leukemia (ALL) are common. It has been reported to occur in up to 90% of patients with this disease. It was observed in 48 of the 50 patients in a study [4]. Leukemic relapses are often diagnosed after the ocular presentation. The ocular involvement has been associated with higher frequency of bone marrow relapses and central nervous system compromise weeks or months later, which means a poor prognosis and low survival rate.
A lot of lesions are asymptomatic and patients are diagnosed during routine examination by ophthalmologist [5]. Therefore it is important to consider fundoscopic evaluation at the time of diagnosis of leukemia. Ophthalmic involvement in acute lymphoblastic leukemia can be classified into two major categories: primary or direct leukemic infiltration of the ocular structures and secondary or indirect involvement. These secondary changes may be the result of hematological abnormalities such as anemia, thrombocytopenia, leucopenia, and hyperviscosity. Likewise, opportunistic infections due to immunosuppression particularly viral, protozoal and fungal infections and the leukemia treatment itself may secondarily involve the ocular system [6]. Previous studies revealed optic disc edema, dilated and tortuous retinal vessels, retinal blot and flame shaped hemorrhages, Roth’s spot, perivascular sheathing and exudates during fundoscopic examination of leukemic patients [7].
This descriptive, cross-sectional study was carried out in Medicine and Oncology departments of Bangladesh Medical College Hospital from May, 2020 to October 2020. Total 50 known cases of leukemia were selected. The diagnosis was made by bone marrow study in case of acute leukemia’s and chronic myeloid leukemia and by peripheral blood film with immunophenotyping in case of chronic lymphocytic leukemia. Fundoscopic findings and hematological parameters of these diagnosed cases were collected in this study. Fundoscopic examination was reviewed by an ophthalmologist. Collected data was analyzed statistically by using SPSS-17 (Chicago, Illinois).
Inclusion criteria
1. Diagnosed cases of leukemia (AML, ALL, CML, CLL). Diagnosis of acute leukemia will be based on bone marrow evidence and chronic leukemia on Complete Blood count (CBC) and peripheral blood film (PBF) and immunophenotyping in case of CLL.
2. Age more than 16 years.
Exclusion criteria
1. Patients unwilling to participate in this study
2. Patients with coexisting ocular diseases and systemic diseases along with ocular manifestations, e.g. DM, hypertension, retinal vascular disease, sickle cell disease, etc
3. Severely ill patients who were uncooperative for examination
4. Patients with cataract
5. Patients who had already received treatment of leukemia
This descriptive cross sectional study on 50 Leukemic patients was carried out in the in-patients departments of medicine and oncology of Bangladesh Medical College and Hospital (BMCH), Dhaka from May, 2020 to October, 2020 to find out the demographic profile and correlation between fundoscopic findings and hematological parameters of leukemia patients in the tertiary level hospital in Bangladesh.
Figure 1 and table 1 showing the age distribution of 50 leukemic patients. It was obvious that more than 60 years persons were affected more (total 16, 32%) than that of any age group followed by age between 21-30 years (total 14, 28%), between 41-50 years (total 9, 18%), between 31-40 years (total 6, 12%), between 51-60 years (total 3, 6%). Age less than 20 years were the least affected (total 2, 4%).
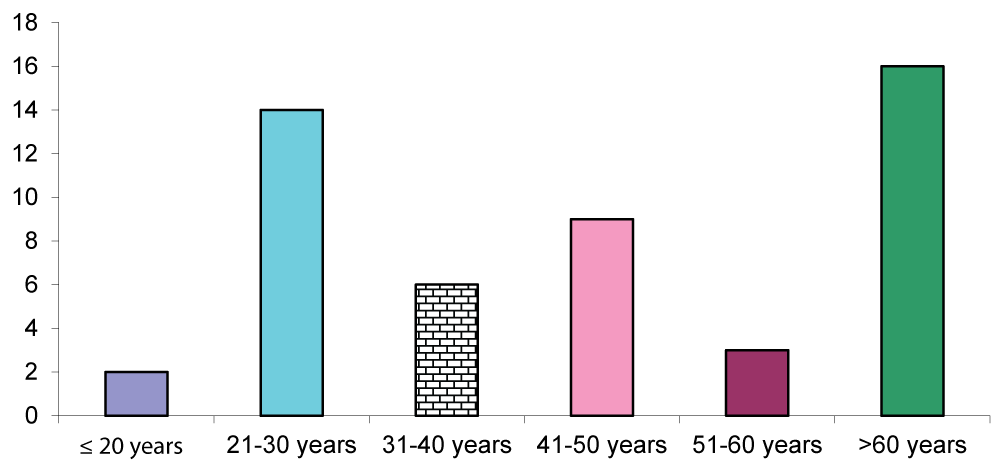
Figure 1: Age group distribution of study population.
| Table 1: Age distribution of study population. | |
| Age(years) | No of patients (%) |
| Less or equal to 20 years | 02(4%) |
| 21-30 years | 14(28%) |
| 31-40 years | 06(12%) |
| 41-50 years | 09(18%) |
| 51-60 years | 03(6%) |
| More than 60 years | 16(32%) |
Figure 2 showing females were affected more (total 26, 52%) than males (total 24, 48%).
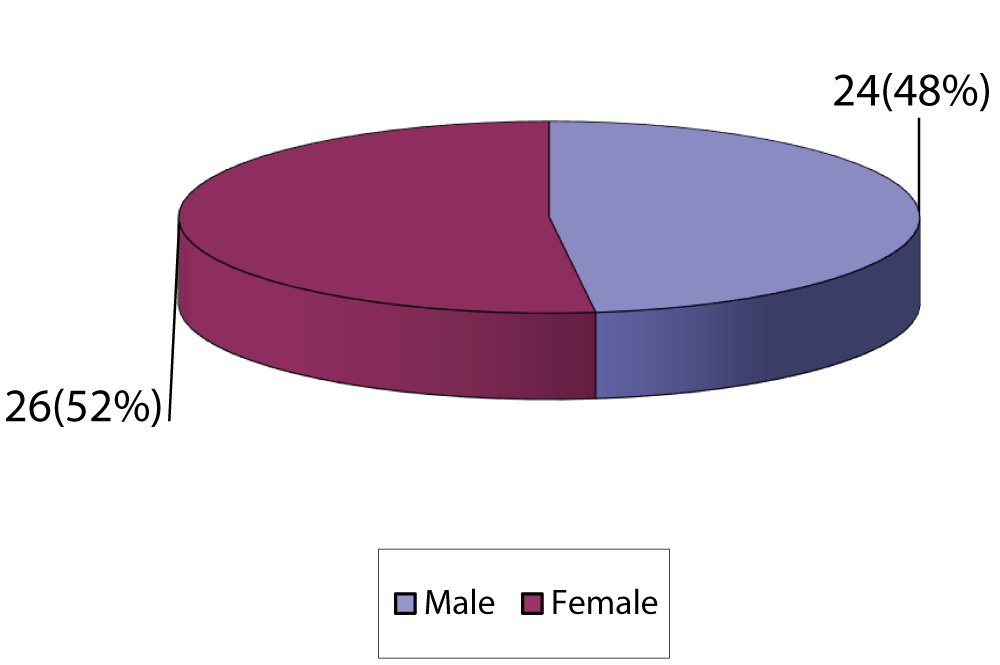
Figure 2: Sex distribution of study population.
Figure 3 showing among the 50 patients, the fundal lesion was detected in 32 patients (64%). Figure 4 showing among 32(64%) patients with fundoscopic abnormalities, only 3 patients (9%) had exudates while others (29, 91%) have retinal hemorrhages. Exudates did not show any statistically significant relationship with types of leukemia (p value = 0.53) Figure 5.
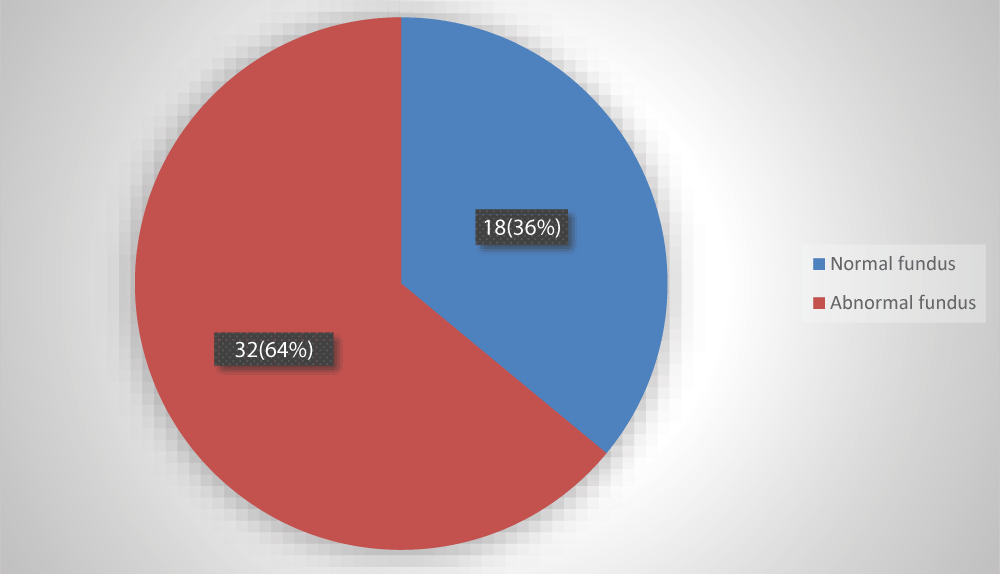
Figure 3: Showing fundoscopic findings in leukemia patients.
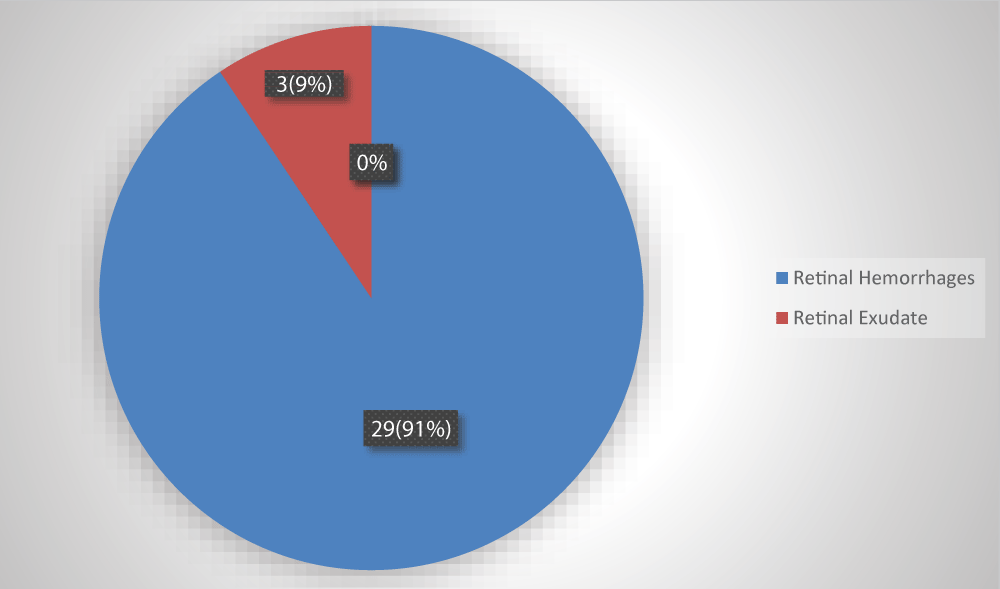
Figure 4: Showing types of fundoscopic abnormalities in leukemia patients.
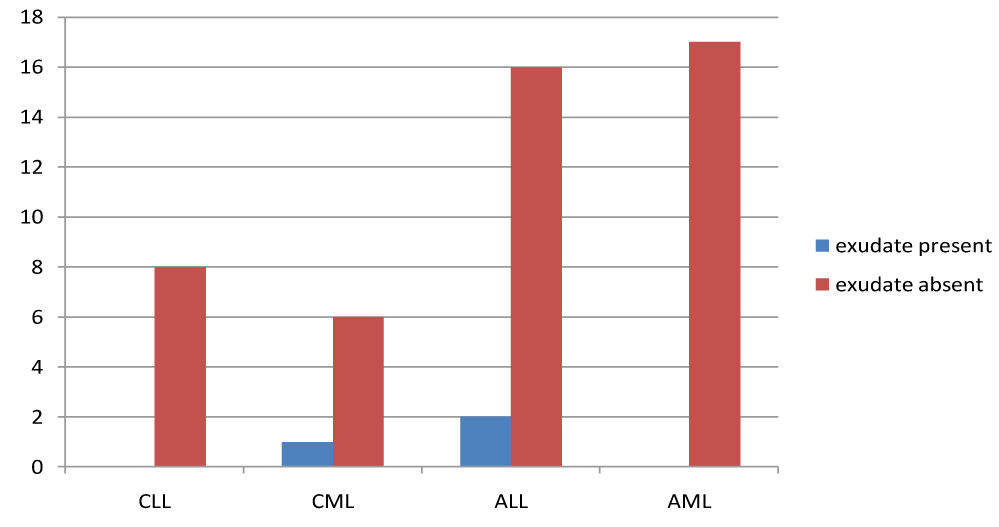
Figure 5: Bar chart shows distribution of exudates in different types of leukemia.
Table 2 shows 3 out of 32 patients with anemia (hemoglobin less than 10 gram/dl) have retinal exudates and 18 out of 18 patients without anemia have no exudates. There were no statistically significant correlation between anemia and retinal exudates (p value > 0.05).
| Table 2: Correlation between Anemia with Exudates. | ||||
| Hb level (gm/dl) | Exudates | |||
| Yes | No | Total | p value | |
| < 10 gm/dl | 03 (100) | 29 (61.7) | 32 | 0.11ns |
| ≥ 10 gm/dl | 00 | 18 (38.30) | 18 | |
| Total | 03 (100) | 47 (100) | 50 | |
Table 3 shows 28 out of 29 patients without high leukocyte count (white blood cell count more than 100000/cmm) have no exudates and only 2 out of 21 patients with high leukocyte count have exudates. P value was > 0.05 which was not statistically significant.
| Table 3: Correlation between high WBC counts with Exudates | ||||
| Total WBC count | Exudates | |||
| Yes | No | Total | p value | |
| ≤ 100000/mm3 | 01(33.33) | 28(59.57) | 29 | 0.56ns |
| > 100000/mm3 | 02(66.67) | 19(61.70) | 21 | |
| Total | 03(100) | 47(100) | 50 | |
Table 4 shows 35 out of 36 patients with thrombocytopenia (platelet count less than 150000/cmm) have no retinal exudates and 2 out of 14 patients without thrombocytopenia have exudates. Statistically significant relation was not found between thrombocytopenia and retinal exudates (p value > 0.05).
| Table 4: Correlation between thrombocytopenia with Exudates | ||||
| Platelet count | Exudates | |||
| Yes | No | Total | p value | |
| ≤ 150000/mm3 | 01(33.33) | 35(74.47) | 36 | 0.18ns |
| > 150000/mm3 | 02(66.67) | 12(25.53) | 14 | |
| Total | 03(100) | 47(100) | 50 | |
Leukemic retinopathy is the term most used to denote fundus manifestations of anaemia, thrombocytopenia and increased blood viscosity seen in patients with leukemia.9In the present study, higher prevalence (64%) of leukemic retinopathy was noted than the prevalence of 42%, 43% and 49% reported by Guyer, et al. [9], Abu, el-Asrar, et al. [13] and SC Reddy and N Jackson [16] respectively. Intra retinal hemorrhages were seen more often than above three studies. This very high percentage of fundoscopic abnormalities may due to majority of patients with acute leukaemia and co-occurrence of thrombocytopenia and anemia in the majority of patients.
In the present study, 28 out of 36 patients with thrombocytopenia have retinal hemorrhages and 13 out of 14 patients without thrombocytopenia have no hemorrhages. Statistically significant relation was found between thrombocytopenia and retinal hemorrhages (p value < 0.05). This finding is consistent with the study finding of “A Prospective Ophthalmic Evaluation of Patients with Acute Myeloid Leukemia: Correlation of Ocular and Hematologic findings” done by Karesh, et al. [3] and Retinopathy in acute leukemia at initial diagnosis: correlation of the fundal lesions and hematological parameters” done by Reddy, Jackson [16]. In contrast another study was done by Abu el-Asar, et al. finds no relation between thrombocytopenia and retinal haemorrhage [13].
In this study, 21 out of 32 patients with anemia have retinal hemorrhages and 10 out of 18 patients without anemia have no hemorrhages. There were no statistically significant correlation between anemia and retinal Hemorrhages (p value > 0.05). However, other researchers have noted an association between anemia and the presence of retinal haemorrhages [14,16]. This finding may be due to small sample size in this study.
Shivaprasad C and Srinivasan R, studied, 120 eyes of 60 consecutive patients with leukemia and lymphoma who presented to the hematology clinic of Jawaharlal Nehru Institute of Postgraduate Medical Education and Research were included in this study. Of the 60 patients examined which included 32 males and 28 females, 36 of them had chronic leukemia, 18 had acute leukemia and 6 patients had lymphomas. Ocular manifestations were present in 42.85% (25 patients). The most common ocular manifestation was conjunctival pallor in 30.95% (18 patients). Retinal changes were seen in 26.19% (16 patients) which included optic disc pallor and retinal vascular changes with hemorrhages and soft exudates. The retinal changes were bilateral and asymmetrical. Patients with optic disc pallor had hemoglobin ranging from 2.0-6 gram%. Of the total 8 patients presenting with retinal hemorrhages and soft exudates, six of them were acute leukemias, one chronic leukemia, another being Non-Hodgkins lymphoma. All of them had reduced platelet count counts ranging from10000 to 59000. The patient with platelet count of 10000 had more retinal hemorrhages which had also involved the macular area. Visual acuity was decreased in 7.1% due to hemorrhage at macula. Correlation between total white cell count, anemia and retinal hemorrhages or cotton wool spots was not observed in their study. No significant association was found between gender and the presence of retinal lesions. Retinal vascular changes with hemorrhages correlated with platelet counts and are commoner in acute leukemias [15].
Hemorrhages of the retina are the most striking feature of leukemia. They tend to occur most commonly at the posterior pole, may be at any level of the retina and may extend into the subretinal or vitreous spaces. Retinal hemorrhages have been described as dot and blot, or flame-shaped or classically as white-centered hemorrhages. It has been proposed that this white center represent platelet fibrin aggregates.or an accumulation of leukemic cells.
In this study, 19 out of 29 patients without high leukocyte count have hemorrhages and 11 out of 21 patients with high leukocyte count have no hemorrhages. P value was > 0.05 which was not statistically significant. Similarly, Holt and Gordon-Smith and Mahneke and Videbaek, describe that the white blood cell count was not related to the occurrence of White Centered Hemorrhage (WCH) [20]. Guyer, et al. found a non-significant trend of leukocytosis in patients with WCH [10]. In contrast this study finding is not consistent with the observation of Gibson 1938 and Abu el-Asrar, et al. [13].
This prospective, observational case series surveyed adult leukemia patients presenting at Tertiary Hospital population of adult Nigerian Africans departments of Hematology/Immunology and Ophthalmology from July 2003 to August 2008. The demographic profile, clinical data from for each individual in the cohort were statistically collated and analyzed. A p < 0.05 was considered as statistically significant. There were 72 participants (45 males and 27 females), aged 32.7 ± 9.8 years (range, 18 years to 72 years). Leukemic ophthalmopathy was present in 77.8% of subjects. The leading ophthalmic manifestations of leukemia were retinal vascular abnormalities in 50.0% of subjects, conjunctival pallor in 27.8% of subjects, sub-conjunctival hemorrhage in 19.4% of subjects and retinal hemorrhage in 16.7% of subjects. Ocular co-morbidity was present in 47.2% of subjects. Vision loss occurred in 37.5% of subjects, of which 32.1% was leukemia related, and the remaining due to ocular co-morbidity. Leukemic ophthalmopathy was more prevalent in chronic leukemia (p < 0.05), frequently affected the ocular posterior segment (p < 0.05), and often resulted from secondary hematologic complications (p < 0.05). There was no gender difference in the prevalence of leukemia (p = 0.0822) or leukemic ophthalmopathy (p = 0.6624). The prevalence of leukemic ophthalmopathy in Enugu is high. It is often associated with significant ocular co-morbidity and vision loss. These have implications for clinicians involved in leukemia management. Early diagnosis and regular ophthalmic examinations are recommended to optimize treatment outcomes [17].
A prospective study of ocular disorders in adult patients with leukemia at the University of Benin Teaching Hospital, Benin City, Nigeria, between July 2004 and June 2008 was conducted. The patients were interviewed and examined by the authors and the ocular findings were recorded. The means, standard deviation, and the Kruskal-Wallis non parametric test was performed. Forty-seven patients with leukemia were seen. Nineteen patients (40.4%) had CLL, 14(29.8%) had CML, 9(19.1%) had AML and 5(10.6%) had ALL. Seven patients (14.9%) had ocular disorders due to leukemia. The ocular disorders due to the leukemia were proptosis in two patients (4.3%), retinopathy in one patient (2.1%), conjunctival infiltration in one patient (2.1%), periorbital edema in one patient (2.1%), retinal detachment in one patient (2.1%), and subconjunctival hemorrhage in one patient (2.1%). There was no significant difference in rate of the ocular disorders in the various types of leukemia (Kruskal-Wallis KW = 4.019; corrected for ties p = 0.2595). One patient (2.1%) was blind from bilateral exudative retinal detachment while 1 patient (2.1%) had monocular blindness from mature cataract. Ophthalmic disorders that are potentially blinding occur in leukemia. Ophthalmic evaluation is needed in these patients for early identification and treatment of blinding conditions [18].
Chronic myeloid leukemia (CML) is a well-studied entity and advances made in diagnosis and treatment has improved the disease outcome. Patients with ophthalmic manifestation of CML have been reported to have lower 5-year survival rates. Hence, recognizing the early fundus changes may improve outcome by allowing earlier diagnosis and treatment. They report a case of a previously healthy 30-year-old Myanmarese male, who presented with a minor visual disturbance, complaining of seeing a ‘black dot’ in his left visual field for the past 1 week. Fundoscopic examination revealed bilateral retinal blot hemorrhages, white-centered hemorrhage, and preretinal hemorrhage over the left fovea. The full blood count and peripheral blood film were abnormal, and bone marrow biopsy confirmed the diagnosis of CML. Cytoreduction therapy was promptly commenced and his symptoms resolved, with improvement in visual acuity. No complications were recorded at 1-year follow-up [21].
The autopsy study by Leonardy, et al. [22] showed a highly significant correlation between ocular leukaemic cell infiltration and white blood cell counts; in a number of cases, leukaemic cells were seen migrating in choroidal vessels or infiltrating perivascularly. It is probable that this mechanism may explain the role of a white blood cell count in the pathogenesis of retinal hemorrages in these patients.
In this study, 35 out of 36 patients with thrombocytopenia have no retinal exudates and 2 out of 14 patients without thrombocytopenia have exudates. Statistically significant relation was not found between thrombocytopenia and retinal exudates (p value > 0.05).
Similar to the observation of Guyer, et al. [10]. I didn’t find any significant association between the presence of cotton-wool spots and hemoglobin level. However, Abu el-Asrar, et al. [16]. reported that ALL patients with cotton-wool spots had significantly lower hemoglobin levels than patients without such lesions. This study showed no statistically significant correlation between Hemoglobin levels with exudates.
It is observed that the mean white cell counts in patients with cotton wool spot (CWS) in AML and ALL groups was higher than in those without CWS, but this was not statistically significant. Abu el-Asrar, et al. [16] found a significantly lower leukocyte count in patients with AML with CWS, and higher leukocyte count in patients with ALL with CWS, while Guyer, et al. [10]. In the present study, there is no statistically significant association between leukocytosis and the presence of CWS.
Cotton-wool spot are often present in patients with leukemia. They are caused by occlusion of precapillary arterioles resulting in retinal ischaemia [23]. This focal ischaemia leads to a blockage of exoplasmic flow within the nerve fibre layer of the retina, with the subsequent deposition of intraaxonal organelles. The reason for this occlusion in leukemia is poorly understood. They may be related to ischaemia secondary to anemia, direct occlusion by leukemic cells and occlusion by platelet fibrin aggregates or sludging resulting from hyperviscosity [24,25].
In this study, mean age of the population was 47.00 (±19.72), lowest being 18 and highest being 82 years, 24(48%) were male and 26(52%) were female.
Reddy and Jackson study reported, a total of 127 patients with acute leukemia were examined for retinal changes, of whom 78 (61%) were male and 49 (39%) were female; 83 (65%) had myeloid leukemia and 44 (35%) had lymphoid leukemia. The mean age of the patients was 34.6 years (range 13-77 years) [16].
This study has identified retinal exudates among patients with leukemia patients. Retinal exudates were rare (6%) in our study group. However a high percentage of patients (64%) with leukemia had fundal lesions. Recognition of retinopathy is important to improve care of leukemia patients because it has impact on the prognosis and overall management of these patients. Therefore an adequate attention should be paid to fundoscopic evaluation while treating leukemic patients.
Limitation of study
The present study did not represent the actual scenario of leukemic retinopathy in Bangladesh because the study was conducted in one tertiary level hospital (Bangladesh Medical College and Hospital (BMCH) in Dhaka city only. Sample size and duration of the study was short. Treatment outcomes were also not assessed because of lack of follow up.
Ethical clearance: Appropriately taken.
- Catovsky D. Chronic lymphocytic leukemias and other leukaemias of immature B and T cells. In: Weatheral DJ, Ledingham JG, Warell DA, eds. Oxford Textbook of Medicine. 3rd ed. Oxford: Oxford University Press. 1996; 3419-3422.
- Gordon KB, Rugo HS, Duncan JL, Irvine AR, Howes EL, et al. Ocular manifestations of leukaemia: Leukaemic infiltration versus infectious process. Opthalmology. 2001; 108: 2293-2300. PubMed: https://pubmed.ncbi.nlm.nih.gov/11733273/
- Karesh JW, Goldman EJ, Reck K, Kelman SE, Lee EJ, et al. A prospective opthalmic evaluation of patients with acute myeloid leukaemia: Correlation of ocular and haematologic findings. J Clin Oncol. 1989; 7: 528-532. PubMed: https://pubmed.ncbi.nlm.nih.gov/2778482/
- Ohkoshi K, Tsiaras WG. Prognostic importance of opthalmic manifestations in childhood leukaemia. Br J Opthalmology. 1992; 76: 651-655. PubMed: https://pubmed.ncbi.nlm.nih.gov/1477038/
- Ribera JM, Ortega JJ. Leucemia linfoide aguda. In: Haematologia. Garcia- Conde J, San Miguel JF, Sierra J, Urbano-Ispizua A, Vicenti V, Vives JL, eds. Aran: Madrid; 2003; 1029-1042.
- Rosenthal AR. Occular manifestations of leukaemia: A review. Opthalmology. 1983; 90: 899-905. PubMed: https://pubmed.ncbi.nlm.nih.gov/6195573/
- Abdul-Rahim AS, Brown SM, Shami MJ. Bilateral retinal haemorrhages in an 18 year old woman. Surv Opthalmology 2002; 47: 590-593. PubMed: https://pubmed.ncbi.nlm.nih.gov/12504742/
- Schachat AP, Markowitz JA, Guyer DR, Burke PJ, Karpe JA, et al. Ophthalmic manifestations of Leukemia. Arch. Ophtalmology 1989; 107: 697-700. PubMed: https://pubmed.ncbi.nlm.nih.gov/2719579/
- Guyer DR, Schachat AP, Vitale S, Markowitz JA, Braine H, et al. Leukemic retinopathy: Relationship between fundus lesions and hematologic parameters at diagnosis.1989; 96: 860-864. PubMed: https://pubmed.ncbi.nlm.nih.gov/2740081/
- Guyer DR, Schachat AP, Vitale S, Markowitz JA, Braine H, et al. Leukemic retinopathy: Relationship between fundus lesions and hematologic parameters at diagnosis.1989; 96: 860-864. PubMed: https://pubmed.ncbi.nlm.nih.gov/2740081/
- Karesh JW, Goldman EJ, Reck K, Kelman SE, Lee EJ, et al. A prospective ophthalmic evaluation of patients with acute myeloid leukemia: correlation of ocular and hematologic findings. J Clin Oncol. 1989; 7: 1528-1532. PubMed: https://pubmed.ncbi.nlm.nih.gov/2778482/
- Shivaprasad C, Srinivasan R. Ocular Manifestations of Lymphoreticular Disorders. AIOC. 2010; 410-411.
- Abu el-Asrar AM, al-MomSen AK, Kangave D, Harakati MS, Ajarim DS.Correlation of fundus lesions and hematologic findings in leukemic retinopathy. Eur J Ophthalmol.1996; 6: 167-172. PubMed: https://pubmed.ncbi.nlm.nih.gov/8823591/
- Boniface IE, Godswill O, Ibegbulam, S. Ocheni. Ophthalmic Manifestations of Leukemia in a Tertiary Hospital Population of Adult Nigerian Africans. Middle East African J Ophthalmol. 2010; 17: 325–329. PubMed: https://pubmed.ncbi.nlm.nih.gov/21180433/
- Omoti AE, Omoti CE, Momoh RO. Ocular Disorders in Adult Leukemia Patients in Nigeria. Middle East Afr J Ophthalmol. 2010; 17: 165–168. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2892134/
- Reddy SC, and Jackson N. Retinopathy in acute leukaemia at initial diagnosis: correlation of fundus lesions and haematological parameters. Acta Ophthalmol. 2004; 82: 81–85. PubMed: https://pubmed.ncbi.nlm.nih.gov/14738490/
- Huang PK, Sanjay S. Visual Disturbance as the first Symptom of Chronic Myeloid Leukemia. Middle East Afr J Ophthalmol. 2011; 18: 336–338. PubMed: https://pubmed.ncbi.nlm.nih.gov/22224030/
- Duane TD, Osher RH, Green WR. White centered haemorrhages: their significance. Ophthalmology. 1980; 87: 66-69. PubMed: https://pubmed.ncbi.nlm.nih.gov/7375087/
- Allen RA, Straatsma BR. Ocular involvement in leukaemia and allied disorders. Arch Ophthalmol.1961; 66: 490–508. PubMed: https://pubmed.ncbi.nlm.nih.gov/13860566/
- Holt JM, Gordon-Smith EC. Retinal abnormalities in diseases of the blood. Br J Ophthalmol. 1969; 53: 145–160. PubMed: https://pubmed.ncbi.nlm.nih.gov/5252200/
- McLeod D, Marshall J, Kohner EM, Bird AC. The role of axoplasmic transport in the pathogenesis of retinal cotton-wool spots. Br J Ophthalmol. 1977; 61: 177–191. PubMed: https://pubmed.ncbi.nlm.nih.gov/66930/
- Leonardy NJ, Rupani M, Dent G, Klintworth GK. Analysis of 135 autopsy eyes for ocular involvement in leukaemia. Am J Ophthalmol. 1990; 109: 436–444. PubMed: https://pubmed.ncbi.nlm.nih.gov/2330946/
- Kincaid MC, Green WR. Ocular and orbital involvement in leukaemia. Surv Ophthalmol. 1983; 27: 211–232. PubMed: https://pubmed.ncbi.nlm.nih.gov/6342189/
- Ashton N, Henkind P. Experimental occlusion of retinal arterioles. Br J Ophthalmol. 1965; 49: 225–234. PubMed: https://pubmed.ncbi.nlm.nih.gov/14290868/
- Loewenstein JI. Retinopathy associated with blood abnormalities. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. 2. Philadelphia: WB Saunders. 1994; 995–1000.