
More Information
Submitted: July 15, 2022 | Approved: July 27, 2022 | Published: July 28, 2022
How to cite this article: Neokleous N, Mpountola S, Perifanis V. The “sweet” relations between diabetes and platelets. J Hematol Clin Res. 2022; 6: 001-003.
DOI: 10.29328/journal.jhcr.1001019
Copyright License: © 2022 Neokleous N, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

The “sweet” relations between diabetes and platelets
Nikolaos Neokleous* , Stavroula Mpountola and Vasileios Perifanis
, Stavroula Mpountola and Vasileios Perifanis
Department of Preparatory Internal Medicine, AHEPA, Aristotle School of Medicine, Thessaloniki, Greece
*Address for Correspondence: Nikolaos Neokleous, MD, Department of Preparatory Internal Medicine, AHEPA, Aristotle School of Medicine, Thessaloniki, Greece, Email: [email protected]
Atherosclerosis is the most important factor that leads to the high risk of atherothrombotic cases in patients with diabetes mellitus (DM). High morbidity and mortality in these patients are firstly caused by cardiovascular disease, mostly coronary artery disease (CAD) along with acute coronary syndrome (ACS) [1]. It is reported 20 years ago that patients with DM but without CAD have similar cardiac-related mortality risk to patients without DM with myocardial infarction (MI) history [2]. Moreover, cardiovascular disease has a poorer prognosis in patients with DM than the non-DM patients due to the increased risk of complications and recurrent atherothrombotic events [3]. Actually, in an ACS situation, the DM patient has a high possibility to have recurrent ischaemic events and finally die [4]. After all, the presence of several factors and comorbidities has a negative impact on ACS outcomes in DM patients [5]. The increased coagulation along with impaired fibrinolysis, endothelial dysfunction, and platelet hyperreactivity are the main factors that are involved in the prothrombotic condition of DM patients [6,7]. Among them, platelet hyperreactivity is of particular importance, since thrombi formed, developed and sustained with the platelet’s crucial contribution [8]. Platelets of DM patients are becoming hyperreactive, by dysregulation of several signaling pathways, leading to intensified adhesion and aggregation [6,9-12]. Additionally, a hyperreactive platelet may end in an unsatisfactory response to antiplatelet agents [13,14]. Several factors such as hyperglycemia, insulin deficiency resistance, other associated metabolic conditions, and cellular abnormalities (Table 1) intrigue multiple mechanisms that cause the increased platelet reactivity seen in patients with DM [15]. Furthermore, inflammatory activity plays an important role in diabetes and platelet dysfunction. IL-1β secreted by inflammatory cells causes changes to platelet function due to their binding to platelets. This cytokine is critically involved in abnormal clot formation, erythrocyte pathology, and platelet hyper-activation [16].
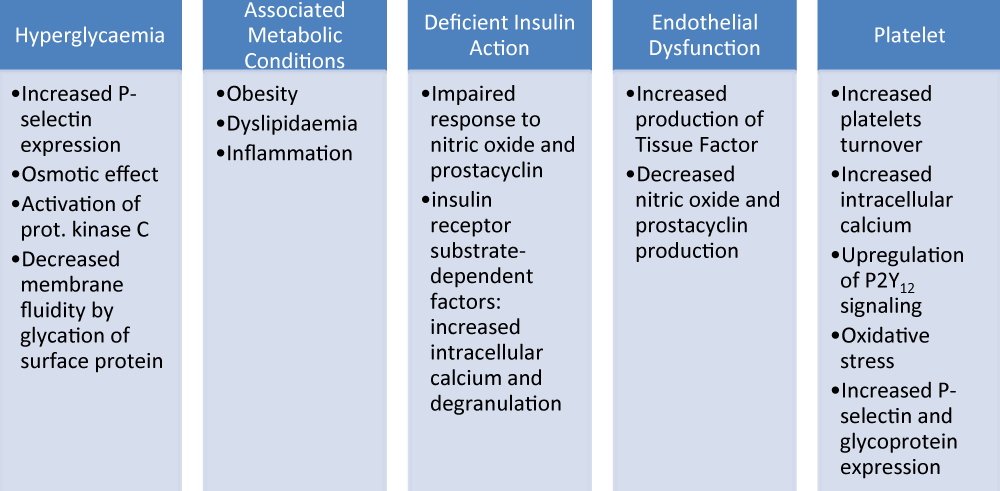
Table 1: ShowingMechanisms contributing to platelet dysfunction in patients with diabetes mellitus (DM).
The fact that the platelet function can be modified in many ways by the diabetic environment explains the failure of glycaemic control alone to decrease the risk of atherothrombotic events in DM patients. Indeed, the increased platelet hyperreactivity is the result of complex inter-regulated pathways (Figure 1). Additionally, bearing in mind that DM platelets show resistance to antiplatelet therapy, it is necessary to find new therapeutical approaches to correct platelet function in diabetes. The comprehension of the molecular pathways that lead to platelet hyperreactivity in DM patients may put the basis for targeted antiplatelet treatment strategies in this high-risk cohort. For example, the fact that calpain, which is elevated in DM patients, plays a significant role in platelet activation, makes it attractive to suggest the Ca2+- activated proteases as a favorable therapeutic target to inhibit thrombotic complications in DM patients.
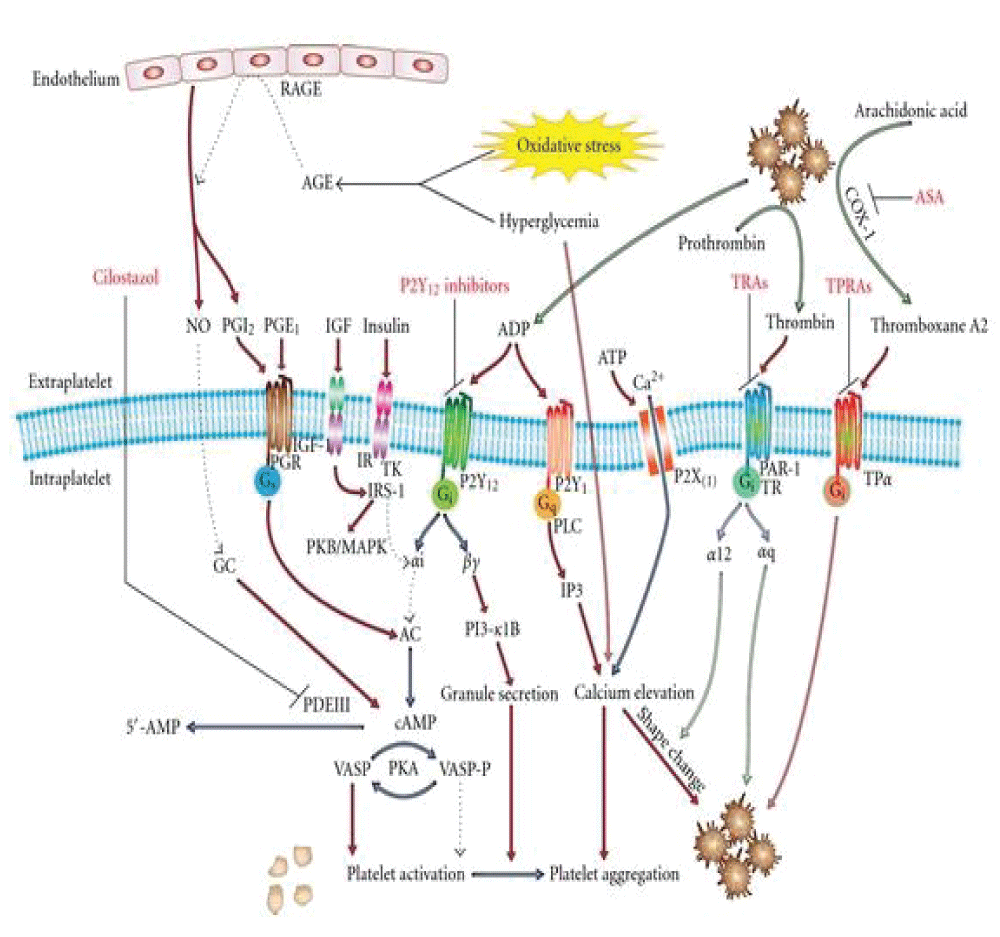
Figure 1: Molecular Pathways that lead to platelet hyperreactivity in DM patients and related possible therapeutic targets.
On behalf of Assistant professor Dr. Vasileios Perifanis, we thank Mrs Susan Lee for the kind invitation to contribute a mini-review to your following volume. It is an honor for us to have your journal as a step to showing our studies to the medical world.
- Webster MW, Scott RS. What cardiologists need to know about diabetes. Lancet. 1997 Jul;350 Suppl 1:SI23-8. doi: 10.1016/s0140-6736(97)90025-8. PMID: 9250280.
- Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998 Jul 23;339(4):229-34. doi: 10.1056/NEJM199807233390404. PMID: 9673301.
- Lüscher TF, Creager MA, Beckman JA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: Part II. Circulation. 2003 Sep 30;108(13):1655-61. doi: 10.1161/01.CIR.0000089189.70578.E2. PMID: 14517152.
- Roffi M, Chew DP, Mukherjee D, Bhatt DL, White JA, Heeschen C, Hamm CW, Moliterno DJ, Califf RM, White HD, Kleiman NS, Théroux P, Topol EJ. Platelet glycoprotein IIb/IIIa inhibitors reduce mortality in diabetic patients with non-ST-segment-elevation acute coronary syndromes. Circulation. 2001 Dec 4;104(23):2767-71. doi: 10.1161/hc4801.100029. PMID: 11733392.
- Brogan GX Jr, Peterson ED, Mulgund J, Bhatt DL, Ohman EM, Gibler WB, Pollack CV Jr, Farkouh ME, Roe MT. Treatment disparities in the care of patients with and without diabetes presenting with non-ST-segment elevation acute coronary syndromes. Diabetes Care. 2006 Jan;29(1):9-14. PMID: 16373888.
- Creager MA, Lüscher TF, Cosentino F, Beckman JA. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: Part I. Circulation. 2003 Sep 23;108(12):1527-32. doi: 10.1161/01.CIR.0000091257.27563.32. PMID: 14504252.
- Osende JI, Badimon JJ, Fuster V, Herson P, Rabito P, Vidhun R, Zaman A, Rodriguez OJ, Lev EI, Rauch U, Heflt G, Fallon JT, Crandall JP. Blood thrombogenicity in type 2 diabetes mellitus patients is associated with glycemic control. J Am Coll Cardiol. 2001 Nov 1;38(5):1307-12. doi: 10.1016/s0735-1097(01)01555-8. PMID: 11691500.
- Davì G, Patrono C. Platelet activation and atherothrombosis. N Engl J Med. 2007 Dec 13;357(24):2482-94. doi: 10.1056/NEJMra071014. PMID: 18077812.
- Stratmann B, Tschoepe D. Pathobiology and cell interactions of platelets in diabetes. Diab Vasc Dis Res. 2005 Feb;2(1):16-23. doi: 10.3132/dvdr.2005.001. PMID: 16305068.
- Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, Ramírez C, Sabaté M, Jimenez-Quevedo P, Hernández R, Moreno R, Escaned J, Alfonso F, Bañuelos C, Costa MA, Bass TA, Macaya C. Platelet function profiles in patients with type 2 diabetes and coronary artery disease on combined aspirin and clopidogrel treatment. Diabetes. 2005 Aug;54(8):2430-5. doi: 10.2337/diabetes.54.8.2430. PMID: 16046311.
- Vinik AI, Erbas T, Park TS, Nolan R, Pittenger GL. Platelet dysfunction in type 2 diabetes. Diabetes Care. 2001 Aug;24(8):1476-85. doi: 10.2337/diacare.24.8.1476. PMID: 11473089.
- Ferroni P, Basili S, Falco A, Davì G. Platelet activation in type 2 diabetes mellitus. J Thromb Haemost. 2004 Aug;2(8):1282-91. doi: 10.1111/j.1538-7836.2004.00836.x. PMID: 15304032.
- Angiolillo DJ. Antiplatelet therapy in diabetes: efficacy and limitations of current treatment strategies and future directions. Diabetes Care. 2009 Apr;32(4):531-40. doi: 10.2337/dc08-2064. PMID: 19336638; PMCID: PMC2660456.
- Natarajan A, Zaman AG, Marshall SM. Platelet hyperactivity in type 2 diabetes: role of antiplatelet agents. Diab Vasc Dis Res. 2008 Jun;5(2):138-44. doi: 10.3132/dvdr.2008.023. PMID: 18537103.
- Ferreiro JL, Angiolillo DJ. Diabetes and antiplatelet therapy in acute coronary syndrome. Circulation. 2011 Feb 22;123(7):798-813. doi: 10.1161/CIRCULATIONAHA.109.913376. PMID: 21343595.
- Bester J, Pretorius E. Effects of IL-1β, IL-6 and IL-8 on erythrocytes, platelets and clot viscoelasticity. Sci Rep. 2016 Aug 26;6:32188. doi: 10.1038/srep32188. PMID: 27561337; PMCID: PMC4999875.