
More Information
Submitted: January 30, 2023 | Approved: February 15, 2023 | Published: February 16, 2023
How to cite this article: Beinema MJ, Brouwers JRBJ, Adriaansen H, Jansman FGA. Prospective evaluation of a computerized algorithm for Vitamin K antagonist drug dose calculation. J Hematol Clin Res. 2023; 7: 001-005.
DOI: 10.29328/journal.jhcr.1001020
Copyright License: © 2023 Beinema MJ, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Prospective evaluation of a computerized algorithm for Vitamin K antagonist drug dose calculation
Maarten J Beinema1*, Jacobus RBJ Brouwers2, Henk Adriaansen3 and Frank GA Jansman2,4
1Thrombosis Centre Deventer Hospital, Deventer, The Netherlands
2Unit of Pharmacotherapy, Epidemiology & Economics, Groningen Research Institute of Pharmacy (GRIP), University of Groningen, Groningen, The Netherlands
3Department of Clinical Chemistry and Thrombosis Services, Gelre Hospital, Apeldoorn, The Netherlands
4Department of Clinical Pharmacy, Deventer Hospital, Deventer, The Netherlands
*Address for Correspondence: Maarten J Beinema, MD, PhD, Thrombosis Centre Deventer Hospital, PO Box 5001, 7400 GC, Deventer, The Netherlands, Email: [email protected], [email protected]
Introduction: In an earlier study, we described and validated a VKA dose-finding algorithm (B2A), based on a novel bidirectional factor (BF). We designed a prospective study to evaluate the B2A in a daily care setting.
Methods: In this open-label prospective study, we compared the outcomes of the B2A over the year 2020 with the outcomes of the previous year (2019), using regular algorithms. The outcomes were the duration of Time in the Therapeutic Range (TTR), the percentage of automated dose proposals (PAuP) and the percentage of accepted dose proposals (PAcP). The data were obtained from three anticoagulation centers in the Netherlands, in four locations. The outcomes of this study were based on a non-inferiority level.
Results: The TTR over the year 2020 was at least non-inferior compared with the standard of care treatment. The percentage of automated proposals increased in all centers to approximately 96% of all dosages.
Conclusion: The B2A performs non-inferior compared with the existing algorithms and in some aspects even better.
Direct Oral Anticoagulants (DOACs) are nowadays the drugs of choice for the prevention and treatment of most thrombo-embolic diseases [1-4]. Vitamin K Antagonists (VKAs) are prescribed for anticoagulant treatment in selected patients with atrial fibrillation, mechanical heart valves and antiphospholipid syndrome [5,6]. VKAs have a narrow therapeutic window and require monitoring of their anticoagulant activity [7-10]. In addition, frequent dose control and/or adjustments are necessary to optimize safety and efficacy [11-13]. In many countries, VKA dose finding is performed in specialized anticoagulation centers to improve the quality of VKA therapy [14,15]. Despite the expertise available at qualified centers, it is often not possible to increase the quality of VKA therapy. The results of poor VKA therapy are both undertreatments, which may lead to recurrent thrombo-embolic events and overtreatment, with the risk of (major) bleeding. Both risks appeared in the comparisons of VKA treatment with the DOACs. This is the main reason for the preference of DOACs over VKA treatment in several guidelines.
Computerized Decision Support systems (CDS) were designed to improve VKA monitoring and dose-finding [16-20].
In an earlier study, we described and validated a dose-finding algorithm (B2A), based on a novel bidirectional factor (BF) [21]. This BF is a linear transformation of the nonlinear INR. A retrospective study with this B2A, based upon the bidirectional factor (BF), showed similar outcomes compared to VKA dose finding guided by experienced staff in the participating anticoagulation centers.
Improvement of the existing management of VKA treatment could lead to a better quality of control and to decrease in clinical outcomes.
We designed a prospective study to evaluate the B2A in a daily care setting.
Design
The algorithm was built within the two major CDS platforms in the Netherlands (Trodis [distributor ASolutions] and Portavita[ CGM]).
In this open-label prospective study, we compared the outcomes of the B2A over the year 2020 with the outcomes of the previous year (2019). In 2019 the medical staff performed dose finding utilizing the existing CDS algorithms in routine situations and manually in difficult cases. The specialized medical staff of the anticoagulation department evaluated all dosage proposals before they were sent to the patients. The quality of VKA therapy is usually expressed as the Time in Therapeutic Range (TTR) [22].
We hypothesized that the algorithm performance was sufficient if the outcomes were at least comparable in both years concerning the TTR and if the percentage of accepted dose proposals would increase.
The Institutional Review Board of the Isala Clinics (Zwolle, the Netherlands) approved the study.
Outcomes
The outcomes were the duration of Time in the Therapeutic Range (TTR), the percentage of automated dose proposals (PAuP) and the percentage of accepted dose proposals (PAcP). The TTR is predictive for thromboembolic and bleeding complications in patients on VKA. The combination of PAuP and PAcP is a key marker of the quality of the algorithm. If both were comparable in the two years, the algorithm would be capable of making a high number of accepted dosage proposals with a comparable TTR as result.
Data collection
The data were obtained from three anticoagulation centers in the Netherlands, in four locations (note: one center had two locations). Two of the thrombosis centers used the CDS PortaVita® and one uses both Trodis® (ASolutions) and PortaVita® in two locations.
From the three anticoagulation centers datasets were obtained. Each dataset contained the TTR, the percentage of automated dosage proposals, and the percentage of accepted proposals. The dataset does not generate information on an individual patient level because of privacy restrictions by law.
In The Netherlands, the Dutch Medicines Evaluation Board has approved acenocoumarol (Tablet 1 mg) and phenprocoumon (Tablet 3 mg): Warfarin is not an approved drug in the Netherlands. Therefore, we analyzed the B2A for both acenocoumarol and phenprocoumon.
Statistical analysis
We determined the combined TTR values of all patients in the four participating centers over the years 2019 and 2020. Furthermore, we compared the percentage of automated proposals (PAuP) and the percentage of accepted proposals (PAcP) over these years.
The outcomes of this study are based on a non-inferiority level [23,24]. The study has an open-label design and the study population could alter over consecutive years. If the outcomes of the B2A were lower compared to the standard method of treatment, the delta value for the statistical testing would be 4%.
We used MedCalc® software for statistical analysis. If the results of the B2A were lower than the results of the existing software we would do several statistical tests in order to analyze this finding. If the outcomes were equal or better, then the outcome would be that the B2A was non-inferior.
Datasets were obtained from the three anticoagulation centers (four locations) over the years 2019 and 2020. In 2019 there were 268.214 INR values and in 2020 257.641. This decrease was mainly due to the ongoing transfer of patients from VKA to DOAC. At the end of 2020, there was a small increase in INR measurements on account of the COVID-19 vaccinations.
TTR
Table 1 shows the TTR results over the years 2019 and 2020.
| Table 1: TTR of all patients over the years 2019-2020 of the three centers. | ||
| Center | 2019 | 2020 |
| 1 | 82,1 | 83,3 |
| 2 | 79,2 | 81,8 |
| 3 | 76,1 | 79,3 |
The TTR over the year 2020 was at least non-inferior compared with the standard of care treatment Figure 1.
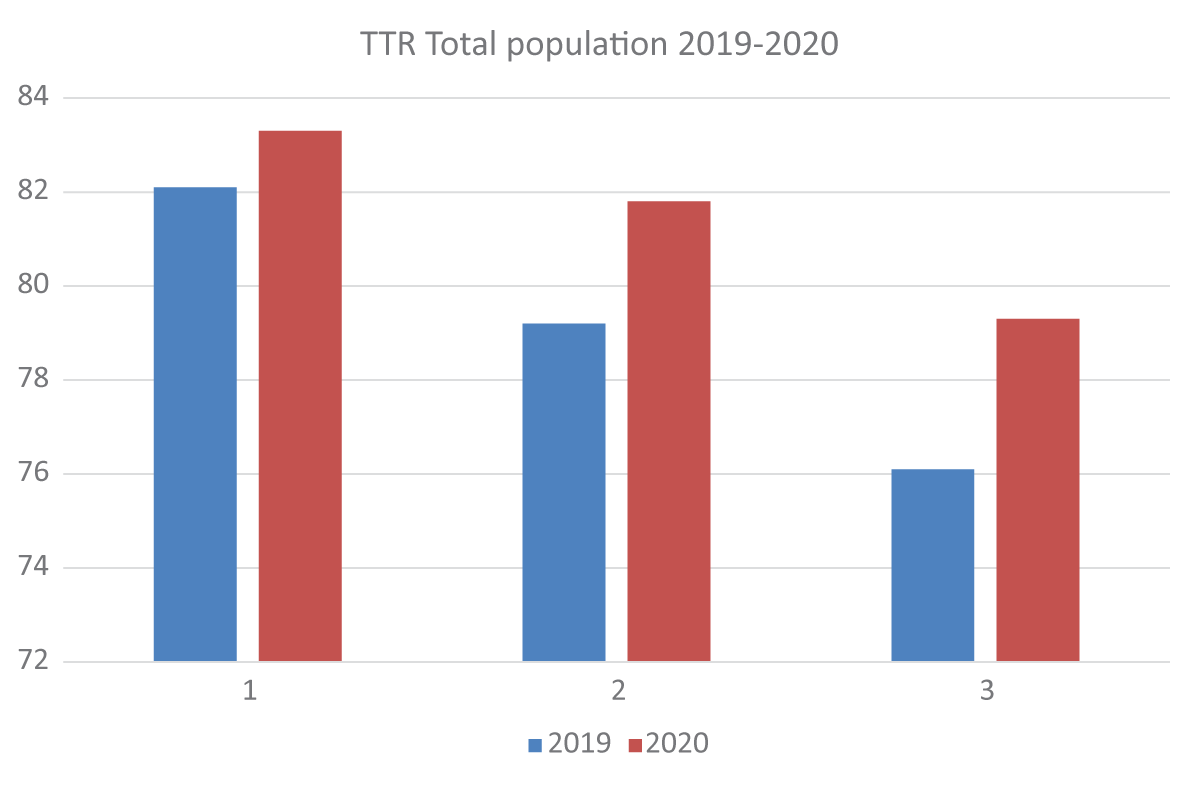
Figure 1: The TTR of all patients over the years 2019-2020 of the three centers.
The percentage of automated proposals (PAuP) and the percentage of accepted proposals (PAcP).
The percentage of automated proposals increased in all centers to approximately 96% of all dosages (Table 2, Figure 2).
| Table 2: The percentage of automated proposals. | ||
| Center | 2019 | 2020 |
| 1 | 0,85 | 0,96 |
| 2 | 0,87 | 0,95 |
| 3 | 0,88 | 0,96 |
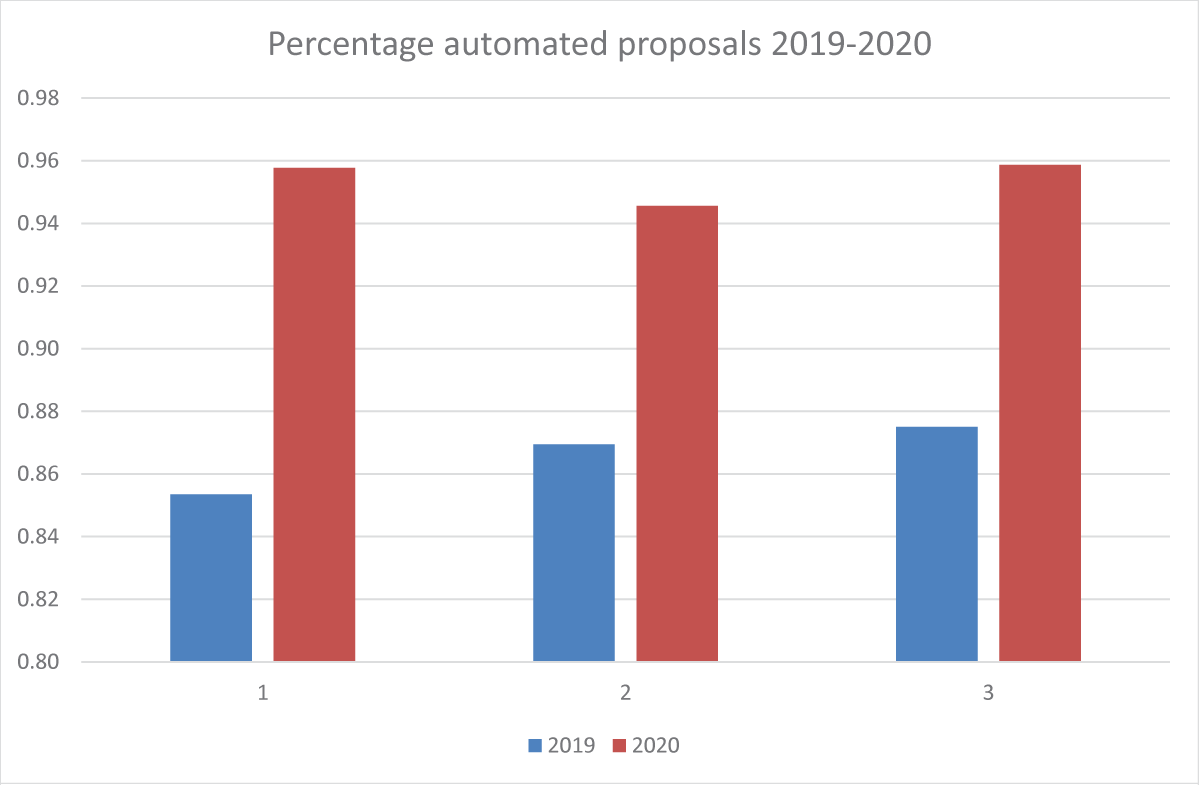
Figure 2: The percentage of automated proposals.
The percentage is never 100% because the B2A only proposes when a former dosage is available. This is not the case with new patients.
The percentage of accepted proposals increased in all centers in subsequent years (Table 3, Figure 3).
| Table 3: Percentage of accepted proposals. | ||
| Center | 2019 | 2020 |
| 1 | 0,72 | 0,76 |
| 2 | 0,78 | 0,82 |
| 3 | 0,82 | 0,88 |
Figure 2: Percentage of accepted proposals.
There are several possible reasons for the alternation of a dosage proposal, for instance, a planned medical intervention or a change of medication intake in the previous period. The percentage of accepted dose advice differs between the three centers, but all centers showed an increase in the percentage of acceptance over the two years.