
More Information
Submitted: April 12, 2023 | Approved: July 01, 2023 | Published: July 03, 2023
How to cite this article: Loriamini M, Lewis-Bakker MM, Binnington B, Kotra LP, Branch DR. Mechanism of Small Molecule Inhibitors of Phagocytosis. J Hematol Clin Res. 2023; 7: 011-014.
DOI: 10.29328/journal.jhcr.1001022
Copyright License: © 2023 Loriamini M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Mechanism of Small Molecule Inhibitors of Phagocytosis
Melika Loriamini1,2, Melissa M Lewis-Bakker3, Beth Binnington2, Lakshmi P Kotra3,4 and Donald R Branch1,2,5*
1Laboratory Medicine and Pathobiology, University of Toronto, Toronto, ON, Canada
2Centre for Innovation, Canadian Blood Services, Toronto, ON, Canada
3Krembil Research Institute, University Health Network, Toronto, Ontario, Canada
4Department of Pharmaceutical Sciences, Leslie Dan Faculty of Pharmacy, University of Toronto, Ontario, Canada
5Department of Medicine, University of Toronto, Toronto, ON, Canada
*Address for Correspondence: Donald R Branch, Laboratory Medicine and Pathobiology, Department of Medicine, University of Toronto, Centre for Innovation, Canadian Blood Services, Toronto, ON, Canada, Email: [email protected]
Immune cytopenias occur when the body produces antibodies that target specific hematopoietic cells, inducing extravascular antibody-mediated phagocytosis by monocyte-macrophages in the spleen and/or liver through activation of Fcγ Receptors (FcγRs). Immune cytopenias include Immune Thrombocytopenia (ITP), Autoimmune Hemolytic Anemia (AIHA), Hemolytic Transfusion Reactions (HTR), Hemolytic Disease of the Fetus and Newborn (HDFN), and Autoimmune Neutropenia (AIN). Thus, novel therapeutics that inhibit phagocytosis would be useful, especially for short-term use while other therapies are being evaluated. In our earlier studies, we successfully identified two small-molecule drugs able to inhibit in vitro phagocytosis with a low IC50 concentration and negligible toxicity. These drugs, known as KB-151 and KB-208, have the potential to be utilized as lead compounds for further studies, once their mechanism of action is more clearly understood. In this regard, we have developed preliminary results that suggest that these small molecules may bind to the Fc receptors on monocyte macrophages and block the subsequent attachment of antibody-opsonized red blood cells to prevent phagocytosis.
Individuals with immune cytopenias produce antibodies against certain hematopoietic cells in their blood [1-3]. Under these conditions, antibodies coat cells, allowing mononuclear phagocytes to recognize them through their surface Fc Receptors (FcR). Extravascular hemolysis occurs in the spleen and/or liver macrophages after recognition of the opsonized antibodies Fc region by the monocyte-macrophage FcRs, known as antibody-mediated phagocytosis [2]. The process can result in severe and potentially fatal complications for those who are affected [2]. The various types of immune cytopenias can be classified into six categories, which include autoimmune and alloimmune cytopenias [2]. Autoimmune cytopenias include: (i) Immune thrombocytopenia (ITP), which is characterized by specific autoantibodies to platelets, with increased platelet destruction in the spleen and liver, as well as decreased platelet production in the bone marrow; (ii) Autoimmune hemolytic anemia (AIHA), which involves the phagocytosis of autoantibody-coated red blood cells; and (iii) Autoimmune neutropenia (AIN), a rare disorder associated with autoantibodies produced against neutrophils that mainly affects children. Examples of alloimmune cytopenias include: (i) Hemolytic transfusion reaction (HTR), which occurs due to the phagocytosis of donor red blood cells as a result of preformed hemolytic alloantibodies to the donor red cell antigens; (ii) Delayed hemolytic transfusion reaction (DHTR), where the development of hemolytic alloantibodies occurs due to an anamnestic response to a transfusion due to a previous sensitization that is undetectable pre-transfusion; and (iii) Hemolytic disease of the fetus and newborn (HDFN), caused by maternal hemolytic IgG antibodies crossing the placenta into the baby’s circulation and able to destroy baby’s red blood cells.
Destruction via lysis within monocyte-macrophages of specific blood cells opsonized with antibodies is a hallmark of immune cytopenias and requires FcR-mediated phagocytosis. Nevertheless, the elucidation of novel mechanisms to mitigate phagocytosis would offer abeneficial therapeutic intervention [3-5]. Prior studiesfrom our laboratory have documented the chemical synthesis and assessment of multiple small molecules as potentially useful therapeutics for the treatment of ITP, and possibly other immune cytopenias [6,7]. More recently, we have identified two small molecules that exhibit minimal toxicity and significant efficacy in inhibiting in vitro phagocytosis [5]. To obtain preliminary information regarding the mechanism of the inhibition, we examined the ability of these two molecules, KB-151 and KB-208, to inhibit FcR-mediated attachment of antibody-opsonized red blood cells.
Rosette assay
Using a variation of the established monocyte monolayer assay [8,9], PBMCs containing monocytes were allowed to adhere to chamber slides after 1 hr and 30 min at 37 °C with 5% CO2 [8]. As previously reported, KB-151 and KB-208 were dissolved in 100% DMSO and adjusted to a final concentration of 100 µM in RPMI [5]. Following a one-hour incubation period, anti-RhD-opsonized red blood cells with Rh-positive antigens were introduced into the chamber slides. The slides were subsequently incubated for varying durations of 0, 5, 15, 30, 45, and 60 minutes at room temperature. Room temperature incubation allows for the antibody-opsonized red blood cells to attach to the monocytes FcRs but not be phagocytosed, forming so-called rosettes [10]. Following this, the samples were fixed and observed under phase-contrast microscopy to assess the formation of rosettes. Untreated cells were used as our control for rosette formation and as a positive control for inhibition, IVIG, known to inhibit phagocytosis due to the blocking of FcγRs, was used [5,8]. Inhibition of rosettes formation was started after 15 min and completed after 30 min (Figure 1). The inhibition of phagocytosis after the rosettes formation was evaluated by adding 100 µM of KB-151 and KB-208 to the adhered monocytes at room temperature and incubating for 1 hour at 37 °C with 5% CO2 (Figure 2). The number of phagocytosed RBCs in 300 monocytes was used to calculate the phagocytosis index (PI = (# of phagocytosed RBCs/300 monocytes) × 100) [5].
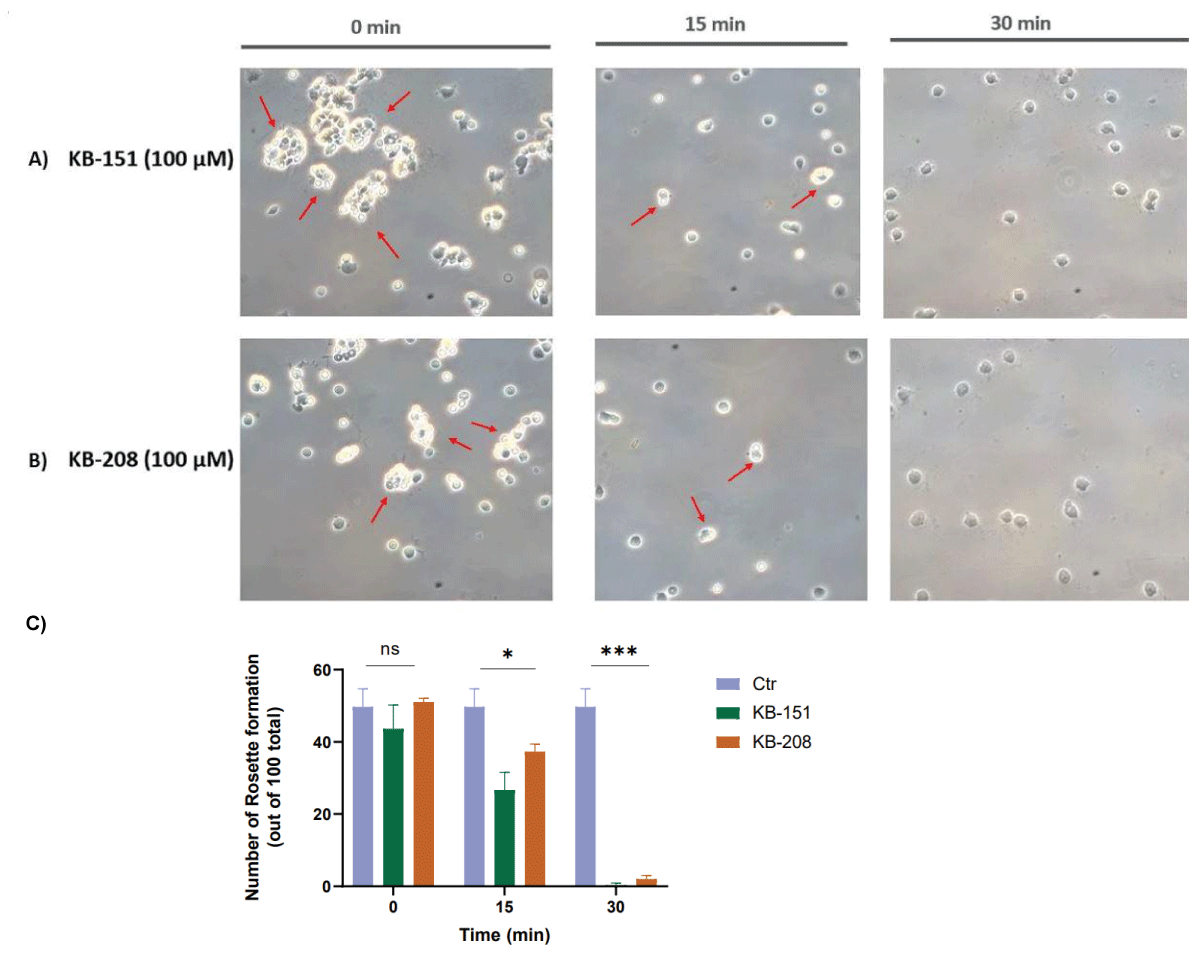
Figure 1: Rosettes formation under phase contrast microscopy- MMA was done at room temperature so as not to allow for phagocytosis which results in RBC rosettes forming; e.g., only attachment of anti-D-opsonized RBCs. (A) Human monocytes treated with KB-151 at 100 µM concentration for 0-, 15-, and 30-min. Rosettes formation (red arrow) started to be inhibited after 15 min and was completely inhibited after 30 min. (B) Human monocytes were treated with KB-208 at 100 µM concentration for 0-, 15-, and 30-min. Rosette formation started to be inhibited after 15 min and was completely inhibited after 30 min. (C) The number of rosettes formation. The rosette formation of each field is analyzed. Rosette inhibition began at the 15-minute mark and reached completion at the 30-minute mark. The sample size of n = 3 was utilized to count 100 monocytes in each chamber, which suggests the existence of rosettes.
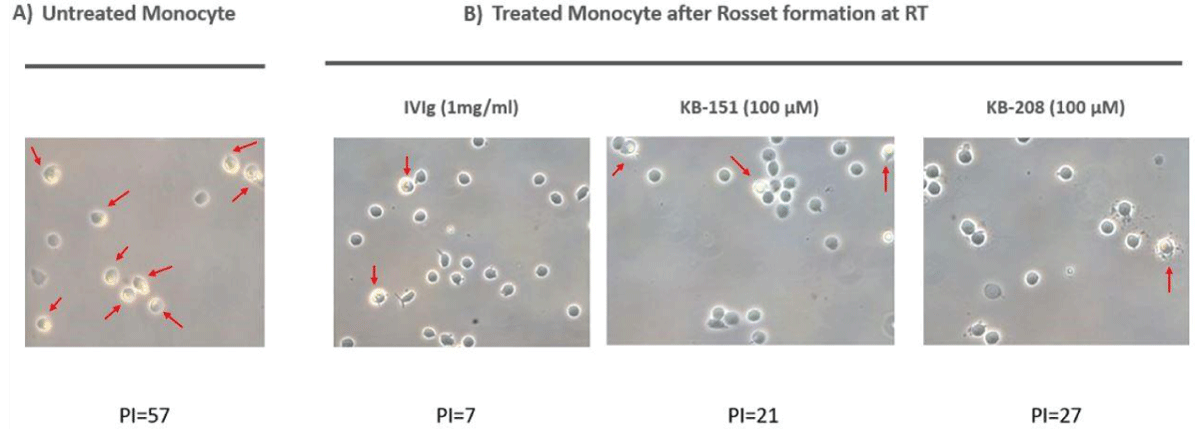
Figure 2: Phagocytosis after rosettes formation under phase contrast microscopy. MMA was done first at room temperature so that rosettes would form; e.g., only attachment of anti-D-opsonized RBCs. Then, the RT MMA was moved to 37 °C and optimal pH for phagocytosis to occur. (A) Untreated human monocytes representing monocytes phagocytosing RBCs opsonized with anti-D, after rosettes formation (Figure 1), moved to 37 °C. (B) Human monocytes pre-treated for 15 min. with IVIg (1 mg/ml), KB-151 (100 µM), and KB-208 (100 µM) prior to moving to 37 °C- representing monocytes now phagocytosing RBCs opsonized with anti-D.
There is a limited number of established treatments for severe manifestations of immune cytopenias. The majority of novel therapies have prioritized the treatment of ITP over other categories of immune cytopenia, including AIHA, HTR, (DHTR), and HDFN. Standard treatments for ITP and AIHA include corticosteroids such as dexamethasone and prednisone, as well as rituximab which is an anti-CD20 medication. Additionally, intravenous immunoglobulin (IVIG) and anti-D treatments are also utilized [11-13]. IVIG is considered second-line therapy for ITP; however, several options exist as alternatives to IVIG, such as thrombopoietin receptor agonists (TPOS-Ras), including Eltrombopag and Avatrombopag, anti-D, Spleen tyrosine kinase (Syk) inhibitors like fostamatinib, and splenectomy [14-18]. The efficacy of current therapies is limited by the time required for their effects to manifest. Consequently, patients with acute ITP, HTR, DHTR, HDFN, and fulminant AIHA, who are at risk of rapid cell destruction are also at risk for high morbidity and mortality. Hence, expeditious interventions that can counteract the immune-mediated eradication of particular blood cells would confer significant benefits. More precisely, they would allocate supplementary time for the execution of alternative therapeutic approaches that would enhance the likelihood of the patient’s improvement and survival. KB-151 and KB-208 significantly inhibited phagocytosis in human monocyte-macrophages at low µM IC50 concentrations with minimal to no toxicity in vitro, up to 250 µM, according to our previous work [5]. In the report herein, we provide preliminary findings that the inhibition of phagocytosis is due to the ability of the two drugs to inhibit the attachment of opsonized RBCs to FcɣRs on the monocytes. In addition, the fact that these small molecules can work to inhibit phagocytosis when the rosetting RBCs at room temperature are moved to optimal conditions for phagocytosis (37 °C and buffered physiologic pH [8]), suggests that these small molecules are able to enter the cells to cause the phagocytosis inhibition. This may indicate that the mechanism of action of these small molecules may be to affect signal transduction pathways. To elucidate the precise mechanism of action, additional studies are required.
- Gilliland BC, Evans RS. The immune cytopenias. Postgrad Med. 1973 Nov;54(5):195-203. doi: 10.1080/00325481.1973.11713621. PMID: 4583297.
- Petz LD, Garratty G. Immune Hemolytic Anemias, 2nd ed.; Petz LD, Garratty G, Eds, Churchill Livingstone: Philadelphia. PA, USA. 2004.
- Connell NT, Berliner N. Fostamatinib for the treatment of chronic immune thrombocytopenia. Blood. 2019 May 9;133(19):2027-2030. doi: 10.1182/blood-2018-11-852491. Epub 2019 Feb 25. PMID: 30803989.
- Zuercher AW, Spirig R, Baz Morelli A, Rowe T, Käsermann F. Next-generation Fc receptor-targeting biologics for autoimmune diseases. Autoimmun Rev. 2019 Oct;18(10):102366. doi: 10.1016/j.autrev.2019.102366. Epub 2019 Aug 9. PMID: 31404703.
- Loriamini M, Lewis-Bakker MM, Frias Boligan K, Wang S, Holton MB, Kotra LP, Branch DR. Small Molecule Drugs That Inhibit Phagocytosis. Molecules. 2023 Jan 12;28(2):757. doi: 10.3390/molecules28020757. PMID: 36677815; PMCID: PMC9867408.
- Purohit MK, Scovell I, Neschadim A, Katsman Y, Branch DR, Kotra LP. Disulfide linked pyrazole derivatives inhibit phagocytosis of opsonized blood cells. Bioorg Med Chem Lett. 2013 Apr 15;23(8):2324-7. doi: 10.1016/j.bmcl.2013.02.064. Epub 2013 Feb 26. PMID: 23489619.
- Purohit MK, Chakka SK, Scovell I, Neschadim A, Bello AM, Salum N, Katsman Y, Bareau MC, Branch DR, Kotra LP. Structure-activity relationships of pyrazole derivatives as potential therapeutics for immune thrombocytopenias. Bioorg Med Chem. 2014 May 1;22(9):2739-52. doi: 10.1016/j.bmc.2014.03.016. Epub 2014 Mar 19. PMID: 24685704.
- Tong TN, Burke-Murphy E, Sakac D, Pendergrast J, Cserti-Gazdewich C, Laroche V, Branch DR. Optimal conditions for the performance of a monocyte monolayer assay. Transfusion. 2016 Nov;56(11):2680-2690. doi: 10.1111/trf.13766. Epub 2016 Aug 21. PMID: 27546234.
- Tong TN, Cen S, Branch DR. The Monocyte Monolayer Assay: Past, Present and Future. Transfus Med Rev. 2019 Jan;33(1):24-28. doi: 10.1016/j.tmrv.2018.07.004. Epub 2018 Aug 8. PMID: 30139679.
- Rampersad GC, Suck G, Sakac D, Fahim S, Foo A, Denomme GA, Langler RF, Branch DR. Chemical compounds that target thiol-disulfide groups on mononuclear phagocytes inhibit immune mediated phagocytosis of red blood cells. Transfusion. 2005 Mar;45(3):384-93. doi: 10.1111/j.1537-2995.2005.04241.x. PMID: 15752156.
- Ghanima W, Godeau B, Cines DB, Bussel JB. How I treat immune thrombocytopenia: the choice between splenectomy or a medical therapy as a second-line treatment. Blood. 2012 Aug 2;120(5):960-9. doi: 10.1182/blood-2011-12-309153. Epub 2012 Jun 26. PMID: 22740443.
- Thompson JC, Klima J, Despotovic JM, O'Brien SH. Anti-D immunoglobulin therapy for pediatric ITP: before and after the FDA's black box warning. Pediatr Blood Cancer. 2013 Nov;60(11):E149-51. doi: 10.1002/pbc.24633. Epub 2013 Jun 27. PMID: 23813881.
- Long M, Kalish LA, Neufeld EJ, Grace RF. Trends in anti-D immune globulin for childhood immune thrombocytopenia: usage, response rates, and adverse effects. Am J Hematol. 2012 Mar;87(3):315-7. doi: 10.1002/ajh.22261. Epub 2011 Dec 21. PMID: 22190130; PMCID: PMC3767405.
- Almizraq RJ, Branch DR. Efficacy and mechanism of intravenous immunoglobulin treatment for immune thrombocytopenia in adults. Ann Blood 2021; 6:2.
- Braselmann S, Taylor V, Zhao H, Wang S, Sylvain C, Baluom M, Qu K, Herlaar E, Lau A, Young C, Wong BR, Lovell S, Sun T, Park G, Argade A, Jurcevic S, Pine P, Singh R, Grossbard EB, Payan DG, Masuda ES. R406, an orally available spleen tyrosine kinase inhibitor blocks fc receptor signaling and reduces immune complex-mediated inflammation. J Pharmacol Exp Ther. 2006 Dec;319(3):998-1008. doi: 10.1124/jpet.106.109058. Epub 2006 Aug 31. Erratum in: J Pharmacol Exp Ther. 2013 May;345(2):326. PMID: 16946104.
- McKeage K, Lyseng-Williamson KA. Fostamatinib in chronic immune thrombocytopenia: a profile of its use in the USA. Drugs Ther Perspect. 2018;34(10):451-456. doi: 10.1007/s40267-018-0551-x. Epub 2018 Aug 29. Erratum in: Drugs Ther Perspect. 2018;34(12):594. PMID: 30459507; PMCID: PMC6223701.
- Cheloff AZ, Al-Samkari H. Avatrombopag for the treatment of immune thrombocytopenia and thrombocytopenia of chronic liver disease. J Blood Med. 2019 Sep 5;10:313-321. doi: 10.2147/JBM.S191790. PMID: 31565009; PMCID: PMC6733339.
- Cohn CS, Bussel JB. Romiplostim: a second-generation thrombopoietin agonist. Drugs Today (Barc). 2009 Mar;45(3):175-88. doi: 10.1358/dot.2009.45.3.1343793. PMID: 19436840.