
More Information
Submitted: June 15, 2023 | Approved: July 04, 2023 | Published: July 05, 2023
How to cite this article: Dodoson BT, Fenomanana J, Ramaminiaina ME, Manantsoa SN, Randriamanantany ZA, et al. Evaluation of the Bone Marrow Aspirate Examination Practice at the University Hospital Andrainjato Fianarantsoa, Madagascar. J Hematol Clin Res. 2023; 7: 015-020..
DOI: 10.29328/journal.jhcr.1001023
Copyright License: © 2023 Dodoson BT, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Bone marrow aspirate; Epidemiology; Haemogram; Quality

Evaluation of the Bone Marrow Aspirate Examination Practice at the University Hospital Andrainjato Fianarantsoa, Madagascar
Bronislaw Tchestérico Dodoson1*, Jocia Fenomanana1, Manevarivo Eddy Ramaminiaina2, Stéphania Niry Manantsoa3, Zely Arivelo Randriamanantany2, Andriamiadana Luc Rakotovao4 and Aimée Olivat Rakoto Alson3
1Medical Biology Laboratory, CHU Andrainjato Fianarantsoa, Madagascar
2Medical Biology Laboratory, CHU Tambohobe Fianarantsoa, Madagascar
3UPFR Hematology, CHU-JRA Antananarivo, Madagascar
4Medical Biology Laboratory, CHU-JRB Antananarivo, Madagascar
*Address for Correspondence: Dr. Bronislaw Tchestérico Dodoson, Medical Biologist, Medical Biology Laboratory, CHU Andrainjato Fianarantsoa, Madagascar, Email: [email protected]
Introduction: The bone marrow aspirate examination is defined as a quantitative and qualitative study of bone marrow cells obtained by puncture and aspiration.
Aim: Our objective was to evaluate the practice of this exam at Andrainjato Fianarantsoa University Hospital in order to improve its diagnostic relevance.
Method: This is a prospective and descriptive cross-sectional study of all bone marrow aspirates performed at the Andrainjato Fianarantsoa University Hospital Madagascar, during 18 months, from January 2021 to June 2022.
Results: Forty-two bone marrow aspirate examinations were performed during the study period, among the 338 requests for hematological analysis received, representing a percentage of 1.26%. The average age of the patients was 32.17 years, with a sex ratio of 2.5. The prescription was of hospital origin in 83.3% of patients, motivated by the disturbance of the blood count in 78.6% of cases. Thirty-three requests were evaluated as relevant prescriptions. Coupled with the realization of the bone marrow examination, the haemograms were pathological in 78.6% of cases. The result of the bone marrow aspirate showed normal marrow cytology (16.7%), reactive marrow (23.8%), pathological marrow (50.0%), and hemodiluted marrow (9.5%). Dysmyelopoiesis (33.3%), multiple myeloma (23.8%), and acute leukemia (19.0%) were the main pathologies found. The difficulties encountered were related to the poor quality of the equipment and the non-availability of other complementary explorations.
Conclusion: The bone marrow aspirate examination is technically feasible at Andrainjato Fianarantsoa University Hospital despite the existence of difficulties. The commitment to the process of continuous improvement of quality would impose the improvement of the technical platform.
The bone marrow aspirate examination is defined as a cytological examination consisting of a quantitative and qualitative analysis of medullary hematopoietic precursors [1]. It is a fundamental examination in the diagnosis and follow-up of most hematological diseases. It is indicated for non-peripheral blood count disturbances or bone pain [2,3]. The success of this exam depends first of all on the pre-analytical stage, i.e. on the relevance of the indication, the quality of the sample, and the quality of the marrow smears [4]. The reading of the bone marrow examination then requires an experienced cytologist who synthesizes the clinical and biological data and the abnormalities observed on the bone marrow aspirate to propose one or more diagnostic hypotheses [5].
In terms of statistics, the practice of bone marrow aspirate examination varies according to each country or region [6-8]. To our knowledge, no data on the frequency of this exam has been reported in Fianarantsoa, a regional capital located 400km from the capital of Madagascar, to date. In the vision and commitment to the process of continuous quality improvement in medical biology laboratories, we conducted this study at the multipurpose laboratory of the University Hospital Andrainjato Fianarantsoa, whose main objective was to evaluate the practice of bone marrow aspirate examination in Fianarantsoa.
This is a prospective, cross-sectional, and descriptive study of all bone marrow examinations performed during 18 months, from January 2021 to June 2022, at the multipurpose laboratory service of the University Hospital Andrainjato (CHU-A) Fianarantsoa, Madagascar. The hospital has eight departments: Medical Biology Laboratory, Anatomical Pathology Laboratory, Pharmacy, Medical Imaging, Paediatrics, Stomatology, Surgery Unit, Gastroenterology and Internal Medicine (GEMI). Together with the Tambohobe University Hospital, it is the two main referral centres for the Haute Matsiatra region and neighbouring regions.
The sampling was done in an exhaustive way, so the study did not exclude any bone marrow aspirate whatever the result obtained, or even in case of a possible problem during its realization.
Regarding bone marrow aspiration, the procedure has always been preceded by physical and psychological preparations which are of capital importance for its success. Then, the standard asepsis was carried out using alcohol and yellow betadine. Due to a lack of technical means, the Mallarmé trocar used was of a single size for all types of patients (child or adult). It was reusable after cold sterilization. After obtaining the medullary juice, it was immediately spread on 6 to 8 glass slides using two techniques: the medullary smear technique and the lump crushing technique. Half of the slides were then stained by May Grunwald Giemsa.
A total of 6,464 test requests were processed in our laboratory during 18 months, with 3,338 hematology test requests recorded, including 42 bone marrow examinations, giving a rate of 1.26%. The demographic characteristics of the patients are summarized in Table 1.
| Table 1: Patient demographics. | ||||
| Parameters | Number (N = 42) | Percentage (T = 100%) | ||
| Age (years old) (Min = 2 ; Max = 71 ; Mean = 32,17) |
0 – 15 | 11 | 26,2 | |
| 15 – 30 | 10 | 23,8 | ||
| 30 – 45 | 8 | 19,0 | ||
| 45 – 60 | 9 | 21,4 | ||
| ≥ 60 | 4 | 9,5 | ||
| Gender | Male | 30 | 71,4 | |
| Female | 12 | 28,6 | ||
The indications are shown in Figure 1. Patients were hospitalized in 83.3% of cases, dominated by the internal medicine department (50.0%) and pediatrics (23.8%).
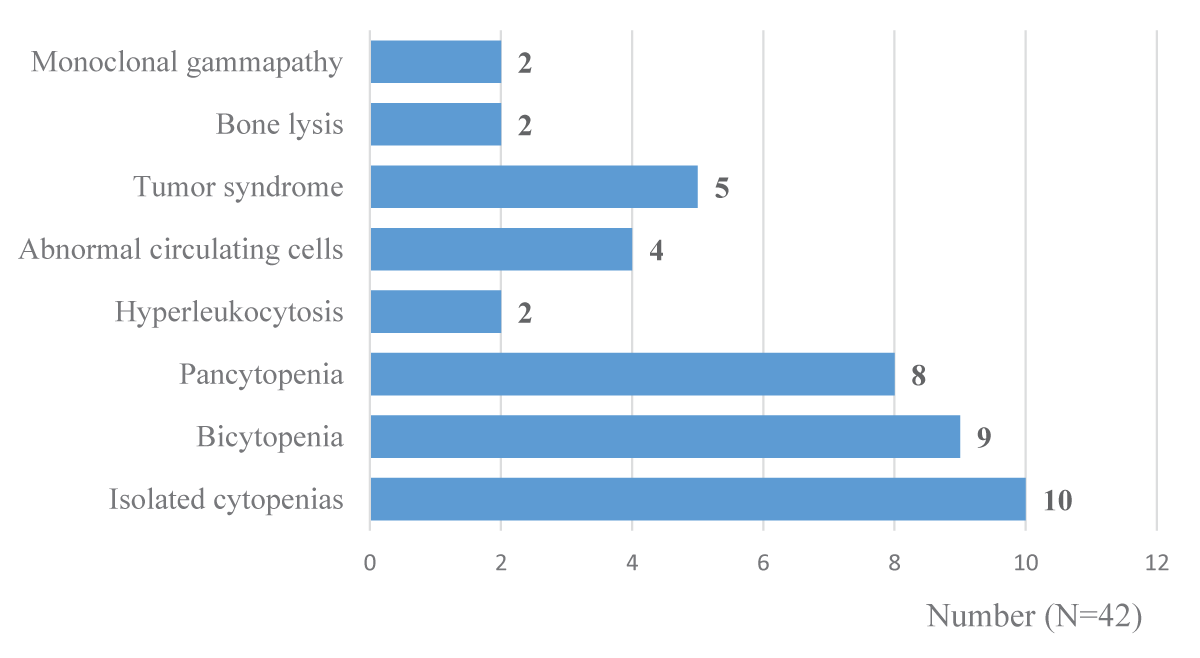
Figure 1: Indications for bone marrow aspirate performed.
All prescriptions issued in due form, which were preceded by a clinical-biological and/or radiological etiological exploration to eliminate peripheral causes, were evaluated as relevant. Thus, nine prescriptions (21.4%) were evaluated as irrelevant in this study.
Regarding bone marrow puncture, the sternal site was preferred in 88.1% of patients. Bone hardness was normal in 30 patients (71.4%). As for the outcome of the samples taken: aspiration was easy in 71.4% of cases, bringing back bone marrow with hematopoietic lumps in most cases. When it was difficult, the quality obtained was significantly lower (no visible lumps).
The overall results of the bone marrow aspirate examination performed are shown in Table 2.
| Table 2: Results of the marrow aspirate performed. | ||
| General result | Appearance | Numbers (N = 42) |
| Normal marrow | Normal cytology | 7 |
| Reactive marrow | Erythroblastic hyperplasia | 5 |
| Granulocytic hyperplasia | 4 | |
| Megakaryocytic hyperplasia | 1 | |
| Pathological marrow | Acute leukemia
|
3 1 |
| Chronic myeloid leukemia | 2 | |
| Multiple myeloma | 5 | |
| Dysmyelopoiesis | 7 | |
| Marrow eosinophilia | 3 | |
| Non-contributory specimen | Bloody marrow | 2 |
| Aspiration without marrow juice | 2 | |
The difficulties encountered were related to the insufficiency of human and material resources due to the non-compliance of the technical platform (absence of complementary explorations such as immunophenotyping, cytogenetics, and molecular biology).
In this study, the 42 bone marrow aspirate examination performed during a period of 18 months represent 1.26% of the hematological analyses performed in the laboratory of the CHU Andrainjato Fianarantsoa. In practice, the bone marrow aspirate is not a routine first-line examination. It seems to be an examination feared by both doctors and patients. However, it is simple and inexpensive to perform [9,10].
A study carried out in another provincial capital in Madagascar showed that 33 bone marrow aspirates were carried out in the laboratory of the PZaGa Mahajanga University Hospital for a period of 18 months [11]. For hospitals with reference centers in hematology, this rate is much higher. Respective averages of 238, 255, and 275 bone marrow examinations per year were performed in Antananarivo, England, and Ivory Coast [12-14].
In our series, the age distribution was quite homogeneous despite a slight predominance of the pediatric population. An average of 32.17 years was found. This average age is similar to the Malagasy studies carried out in Antananarivo and Mahajanga, which found respectively 33.3 and 34.29 years [11,15].
In fact, the age groups that can be concerned with hematological pathologies, explored and/or followed up by bone marrow examination, are variable. Some pathologies, such as acute lymphoblastic leukemia, are more likely to affect children, whereas myeloproliferative and lymphoproliferative syndromes are more likely to affect older subjects [16,17]. The study conducted by El-Hamdaoui in 2018 in Morocco found an average age of 14 years [18], while El Msayryb mentioned an average age of 56 years in his study population performing bone marrow examinations [19]. Thus, various medical specialties, ranging from pediatrics to geriatrics, are concerned by this practice, requiring a clear prioritization of the demand.
Most studies in the literature on marrow aspirate report a predominance of male subjects [12,14,15]. No explanation has been given in the literature. Our results support this hypothesis, since among the total of 42 patients collected, 30 were male and 12 were female, giving a sex ratio of 2.5.
The indications for bone marrow aspirate in our study were dominated by disturbances of the blood count in 78.6% of cases. These results are confirmed by other studies in the literature, highlighting the classic indications for the bone marrow examination that must be mastered by every practitioner. Indeed, the bone marrow examination represents the main exploration of hematopoiesis. A similar study carried out in Ivory Coast found that abnormalities of the hemogram (pancytopenia, bicytopenia, hyperleukocytosis, thrombocytopenia) were the first indication for the bone marrow examination, followed by the assessment of the extension of malignant diseases [14]. Kaur M et al in their studies done in India in 2014 also found that pancytopenia (40%) followed by anemia (38%), came first among the reasons for requesting bone marrow examination [20]. According to Hajiabdolbaghi et al, the bone marrow examination was also indicated in AIDS patients with fever of unknown origin. HIV can interrupt the normal development of bone marrow cell lines [21].
The 9 marrow examination requests received and processed in our laboratory and categorized as “irrelevant prescription” were cases of hypochromic microcytic anemia (4 requests) without prior martial assessment, normochromic normocytic anemia (2 requests) without reticulocyte assay, and suspected multiple myeloma (3 requests) without evaluation of the CRABE criteria in the end, these 9 prescriptions resulted in the bone marrow without cytological abnormalities. These situations could simply be related to a lack of knowledge of the diagnostic approach that should be adopted, making prescribers think first of haemopathies when faced with any abnormality found on the haemogram. The fear would be to miss a hematological malignancy or make a diagnosis too late.
The origin of the prescriptions represented by all kinds of medical disciplines, in hospitals or not, leads us to suggest the interest in standardizing the practical modalities of this examination.
Regarding sampling, the preferred sternal puncture site in 88.1% of the patients in our series is similar to the practices of other authors because of its ease of access and the more comfortable position of the patients in dorsal decubitus, obviously in the absence of contraindication [22,23]. Garrigues P reported in his work that out of 133 bone marrow examinations performed, the preferred puncture site was the sternum in 122 cases (91.7%) [24]. According to our findings, the difficulties of aspiration would be related to extreme ages (young children, elderly subjects), abnormal bone hardness (soft bone), material deficiencies (multiple-use, sterilizable trocar), or simply for undetermined reasons. Thus, it is necessary to anticipate these types of known situations and to adopt preventive measures if possible such as iliac punctures from the outset, the use of trocars adapted to the age, and the professionalisation of practitioners.
For our series of 42 patients, the overall results were classified into 4 distinct types: 7 normal marrows (16.7%), 10 reactive marrows (23.8%), 21 pathological marrows (50.0%) and 4 non-contributory samples (9.5%) were identified. Results similar to ours were reported by Ouattara, et al. in 2000 in Côte d’Ivoire. In their study, 49.69% of pathological, 39.7% of normal, and 10.61% of uninterpretable bone marrow aspirate were seen [14]. Rakotoarivelo ZH et al reported that the overall distribution of bone marrow examination smears in Antananarivo showed 620 normal bone marrow examinations (26.51%), 771 cases (32.91%) of pathological smears, 867 cases (38.68%) of smears showing marrow reactive to peripheral aggression and 82 cases (3.5%) of uninterpretable hemodiluted smears [15]. Loctin A et al. in a study at the University Hospital of Dijon in France between 2005 and 2011, found only 14.1% of pathological bone marrow aspirate in the rheumatology department [25].
The presence of a non-negligible proportion (40.5%) of normal smears and marrow reacting to peripheral damage in our series of cases would suggest a tendency to over-prescribe a bone marrow examination. In case of doubt about the indication or not of a bone marrow examination, a specialized opinion or even a dialogue between clinicians and biologists is necessary in order to establish the right indication.
Among the 21 pathological marrows identified, dysmyelopoiesis (33.3%), multiple myeloma (23.8%), acute (19.0%), and chronic (9.5%) leukemia predominated. Dysmyelopoiesis is manifested by qualitative cytological abnormalities in one or more of the myeloid, erythroid, granular, and megakaryocytic lineages [26]. It should be noted at the outset that dysmyelopoiesis is a cytological symptom and is not synonymous with myelodysplasia. It is an essential criterion for the diagnosis of myelodysplastic syndromes, but it can be observed in other pathologies as well as in various clinical situations where it is generally reversible [27]. In our study, the diagnostic difficulty lay in the differentiation between reactive dysmyelopoiesis and myelodysplastic syndrome. The lack of regular follow-up of the evolution over time, as well as the unavailability of complementary investigations such as Perl’s staining, cytogenetics, and molecular biology, were the causes.
Multiple myeloma was the second most common disease in our series. Multiple myeloma is a malignant B-lymphoid hemopathy, characterized by a clonal proliferation of pathological plasma cells in the bone marrow, secreting complete or incomplete immunoglobulins (Ig) and various cytokines responsible for osteolytic lesions, among other things [28,29]. In our context, the diagnostic problem was the difficulty in obtaining the other clinical-biological and radiological data necessary for the interpretation of bone marrow cytology, but also for the determination of the tumoral or non-tumoral characteristics of the plasma cells observed, since we do not have a technical platform allowing the immunophenotyping of plasma cells.
Acute leukemia refers to a group of malignant proliferation resulting in clonal accumulation in the marrow, blood, and possibly other organs of blood cell progenitors called “blasts”, which have totally or partially lost their ability to differentiate [30,31]. Apart from cytology, our context does not allow for other necessary complementary investigations such as cytochemical staining (Myeloperoxidase, Butyrate-esterase), immunophenotyping of blasts, molecular biology, and cytogenetics.
Our result mentions the discovery of 2 cases in favor of Chronic Myeloid Leukemia (CML), including one case of an 11-year-old child. The diagnosis of CML is confirmed by the presence of the Philadelphia chromosome Ph1 t(9,22) (q34.1;q11.2) and its transcript BCR-ABL1 by cytogenetic and molecular biology examinations [32], which are not currently available in our laboratories.
Hematological diseases represent the third cause of hypereosinophilia after allergic and parasitic diseases [33]. Being a tropical developing country, the main cause of these medullary (and blood) eosinophilias would be parasitosis, followed by allergic diseases [34,35]. Three cases (14.4%) were observed in our series.
In view of the numerous difficulties observed in this study, we will try to propose some practical guidelines to improve the pre-analytical, analytical, and post-analytical phases in the performance of a bone marrow examination.
Concerning the prescription, a form to be filled in by the prescriber must always be used, written in due form. The objective is to collect the maximum amount of information useful to the biologist for the interpretation of the results. Algorithms can be distributed to clinicians to rationalize the prescription. In case of doubt, a specialized opinion or even a dialogue between clinicians and biologists will be necessary.
For the realization of medullary smears, two preparations must be made: the medullary blood smear method and the so-called lump-crushing method [36]. It has been concluded that the lump-crushing technique seems to be more interesting than the smear technique for cell counting (because of the absence of blood dilution effect) and a better evaluation of megakaryopoiesis. However, the smear technique is still more beneficial for the evaluation of total cellularity. The International Council for Standardization in Hematology (ICSH) therefore recommends that slides be prepared systematically using both techniques [8,37].
Finally, concerning the post-analytical phase, the report must be clear, and complete and answer the question(s) asked by the prescriber. It must be co-signed by both biologists. Urgent results (acute leukemia, important bone marrow plasmacytosis, macrophagic activation syndrome, and others) must be communicated as soon as possible by telephone to the prescriber.
The bone marrow aspirate examination has an important place in hematological pathologies as a quantitative and qualitative exploration of the hematopoietic bone marrow. It is an invasive examination that requires specific conditions for its success. Through this evaluation of the practice of bone marrow examination at Andrainjato University Hospital, many technical constraints were raised. Our most relevant suggestions are the absolute necessity to standardize the practical modalities of this examination for the pre-analytical, analytical, and post-analytical phases. These situations would require the commitment and the will of each practitioner and responsible person concerned especially in the improvement of the technical platform to improve the diagnosis and the management of hematological pathologies even at the regional level.
- Tomasian A, Jennings JW. Bone marrow aspiration and biopsy: techniques and practice implications. Skeletal Radiol. 2022 Jan;51(1):81-88. doi: 10.1007/s00256-021-03882-w. Epub 2021 Aug 16. PMID: 34398308.
- Bain BJ. Bone marrow aspiration. J Clin Pathol. 2001 Sep;54(9):657-63. doi: 10.1136/jcp.54.9.657. PMID: 11533068; PMCID: PMC1731527.
- Lucas D. Structural organization of the bone marrow and its role in hematopoiesis. Curr Opin Hematol. 2021 Jan;28(1):36-42. doi: 10.1097/MOH.0000000000000621. PMID: 33177411; PMCID: PMC7769132.
- Riley RS, Hogan TF, Pavot DR, Forysthe R, Massey D, Smith E, Wright L Jr, Ben-Ezra JM. A pathologist's perspective on bone marrow aspiration and biopsy: I. Performing a bone marrow examination. J Clin Lab Anal. 2004;18(2):70-90. doi: 10.1002/jcla.20008. PMID: 15065211; PMCID: PMC6807972.
- Parmentier S, Schetelig J, Lorenz K, Kramer M, Ireland R, Schuler U, Ordemann R, Rall G, Schaich M, Bornhäuser M, Ehninger G, Kroschinsky F. Assessment of dysplastic hematopoiesis: lessons from healthy bone marrow donors. Haematologica. 2012 May;97(5):723-30. doi: 10.3324/haematol.2011.056879. Epub 2011 Dec 16. PMID: 22180437; PMCID: PMC3342975.
- Balasubramanian M, Sangoi NN. Utility of Bone Marrow Examination in Pediatric Age Group: Experience of a Tertiary Healthcare Centre in India. Cureus. 2022 Jul 20;14(7):e27056. doi: 10.7759/cureus.27056. PMID: 36000100; PMCID: PMC9389958.
- Kumar V, Bhatia A, Madaan GB, Marwah S, Nigam AS. Role of Bone Marrow Examination in the Evaluation of Infections: Clinico-Hematological Analysis in a Tertiary Care Centre. Turk Patoloji Derg. 2020;36(1):17-22. English. doi: 10.5146/tjpath.2019.01466. PMID: 31522489.
- Lee SH, Erber WN, Porwit A, Tomonaga M, Peterson LC; International Council for Standardization In Hematology. ICSH guidelines for the standardization of bone marrow specimens and reports. Int J Lab Hematol. 2008 Oct;30(5):349-64. doi: 10.1111/j.1751-553X.2008.01100.x. PMID: 18822060.
- McLenon J, Rogers MAM. The fear of needles: A systematic review and meta-analysis. J Adv Nurs. 2019 Jan;75(1):30-42. doi: 10.1111/jan.13818. Epub 2018 Sep 11. PMID: 30109720.
- Friedrich S, Reis S, Meybohm P, Kranke P. Preoperative anxiety. Curr Opin Anaesthesiol. 2022 Dec 1;35(6):674-678. doi: 10.1097/ACO.0000000000001186. Epub 2022 Sep 21. PMID: 36131642.
- Refeno V, Rakotomalala RS, Rakotonindrina FI, Ahmad Tombovelo V, Rabenandrianina A, Rakoto Alson AO. Epidemiological and clinical description of malignant hemopathies diagnosed in the médullogramme at the Androva University Hospital, Mahajanga. Malagasy Revue de Cancerologie. 2019; 4(1): 949-51.
- Weladji Moukam S. Indications and results of myelograms at the Hematology UPFR of the CHUA-HU-JRA [PhD thesis]. [Faculty of Medicine]: University of Antananarivo; 2015.
- Bain BJ. Bone marrow biopsy morbidity and mortality. Br J Haematol. 2003 Jun;121(6):949-51. doi: 10.1046/j.1365-2141.2003.04329.x. PMID: 12786808.
- Ouattara S, Danho B, Kone M, Tea D. The practice of myelogram at the University Hospital of Treichville: assessment of 19 years of activity. Black African medicine. 2000; 47(5).
- Rakotoarivelo Z, Niry Manantsoa S, Harioly Nirina M, Rakoto Alson AO. Practice of myelogram in 10 years at the Hematology Laboratory of the University Hospital Center Joseph Ravoahangy Andrianavalona (CHUJRA) Antananarivo, Madagascar. Jaccr Africa. 2020; 4(3): 295‑302.
- Rodriguez-Abreu D, Bordoni A, Zucca E. Epidemiology of hematological malignancies. Ann Oncol. 2007 Jan;18 Suppl 1:i3-i8. doi: 10.1093/annonc/mdl443. PMID: 17311819.
- Moueleu Ngalagou PT, Ngouadjeu Dongho Tsakeu E, Ngo Sack F, Eboumbou Moukoko EC, Konn Jolly Y, Luma H. Epidemiology of malignant hemopathies recorded in hospitals in Cameroon. Med Sante Trop. 2018 Feb 1;28(1):61-66. English. doi: 10.1684/mst.2018.0759. PMID: 29616647.
- El-Hamdaoui O. The contribution of the myelogram in the diagnosis of hemopathies: experience of the central hematology laboratory of the Ibn Sina Rabat Hospital [PhD thesis]. [Morocco]; 2018.
- El Msayryb S. Contribution of the myelogram in the diagnosis of hematological malignancies Experience of the hematology department of the Avicenne Marrakech military hospital [Thesis Med]. [Faculty of Medicine and Pharmacy Marrakech]: Cadi Ayyad University; 2020.
- Kaur M, Singh Rana AP, Kapoor S, Puri A. Diagnostic value of bone marrow aspiration and biopsy in routine hematology practice. J Clin Diagn Res. 2014 Aug;8(8):FC13-6. doi: 10.7860/JCDR/2014/9823.4760. Epub 2014 Aug 20. PMID: 25302200; PMCID: PMC4190721.
- Hajiabdolbaghi M, Ataeinia B, Ghadimi F, SeyedAlinaghi S, Badie BM, Dadras O, Rasoolinejad M. Bone Marrow Aspiration/Biopsy in the Evaluation of Fever of Unknown Origin in Patients with AIDS. Infect Disord Drug Targets. 2021;21(3):394-398. doi: 10.2174/1871526520666200705212903. PMID: 32628601.
- Bartakke S, Lukade U, Sethuratnam S. Bone marrow trephine biopsies from posterior superior iliac crest in neonates. Pediatr Blood Cancer. 2021 Apr;68(4):e28893. doi: 10.1002/pbc.28893. Epub 2021 Jan 23. PMID: 33484072.
- Letestu R, Valensi F. La ponction aspiration médullaire à visée diagnostique [Bone marrow aspiration for diagnostic purposes]. Ann Biol Clin (Paris). 2003 Nov-Dec;61(6):655-65. French. PMID: 14711606.
- Philippe G, Licha A. Contribution of the myelogram in internal medicine: study conducted between 2014 and 2018. La Revue de Médecine Interne. 2018; 39: A215.
- Loctin A, Bailly F, Laroche D, Tavernier C, Maillefert JF, Ornetti P. Clinical interest of bone marrow aspiration in rheumatology: a practice-based observational study of 257 bone marrow aspirations. Clin Rheumatol. 2013 Jan;32(1):115-21. doi: 10.1007/s10067-012-2097-y. Epub 2012 Oct 2. PMID: 23053689.
- Germing U, Strupp C, Giagounidis A, Haas R, Gattermann N, Starke C, Aul C. Evaluation of dysplasia through detailed cytomorphology in 3156 patients from the Düsseldorf Registry on myelodysplastic syndromes. Leuk Res. 2012 Jun;36(6):727-34. doi: 10.1016/j.leukres.2012.02.014. Epub 2012 Mar 13. PMID: 22421409.
- Wagner-Ballon O, Imbert M. Dysmyelopoiesis and myelodysplastic syndromes: description – diagnostic approach. Francophone Journal of Laboratories. 2009 ; (413): 39‑47.
- Silberstein J, Tuchman S, Grant SJ. What Is Multiple Myeloma? JAMA. 2022 Feb 1;327(5):497. doi: 10.1001/jama.2021.25306. PMID: 35103765.
- Cowan AJ, Green DJ, Kwok M, Lee S, Coffey DG, Holmberg LA, Tuazon S, Gopal AK, Libby EN. Diagnosis and Management of Multiple Myeloma: A Review. JAMA. 2022 Feb 1;327(5):464-477. doi: 10.1001/jama.2022.0003. PMID: 35103762.
- Rose-Inman H, Kuehl D. Acute Leukemia. Hematol Oncol Clin North Am. 2017 Dec;31(6):1011-1028. doi: 10.1016/j.hoc.2017.08.006. PMID: 29078921.
- Pelcovits A, Niroula R. Acute Myeloid Leukemia: A Review. R I Med J (2013). 2020 Apr 1;103(3):38-40. PMID: 32236160.
- Minciacchi VR, Kumar R, Krause DS. Chronic Myeloid Leukemia: A Model Disease of the Past, Present and Future. Cells. 2021 Jan 10;10(1):117. doi: 10.3390/cells10010117. PMID: 33435150; PMCID: PMC7827482.
- Kovalszki A, Weller PF. Eosinophilia. Prim Care. 2016 Dec;43(4):607-617. doi: 10.1016/j.pop.2016.07.010. Epub 2016 Oct 14. PMID: 27866580; PMCID: PMC5293177.
- van Balkum M, Kluin-Nelemans H, van Hellemond JJ, van Genderen PJJ, Wismans PJ. Hypereosinophilia: a diagnostic challenge. Neth J Med. 2018 Dec;76(10):431-436. PMID: 30569889.
- Savini H, Simon F. Hyperéosinophilie sanguine en zone tropicale [Blood eosinophilia in the tropics]. Med Sante Trop. 2013 May 1;23(2):132-44. French. doi: 10.1684/mst.2013.0187. PMID: 24001638.
- DiFrancesco T, Boychuk DJ, Lafferty JD, Crowther MA. Bone marrow aspirate collection and preparation--a comparison of three methods. Clin Invest Med. 2012 Jun 1;35(3):E114-6. doi: 10.25011/cim.v35i3.16586. PMID: 22673313.
- Lewandowski K, Kowalik MM, Pawlaczyk R, Rogowski J, Hellmann A. Microscopic examination of bone marrow aspirate in healthy adults - comparison of two techniques of slide preparation. Int J Lab Hematol. 2012 Jun;34(3):254-61. doi: 10.1111/j.1751-553X.2011.01387.x. Epub 2011 Dec 7. PMID: 22145778.