
More Information
Submitted: February 27, 2024 | Approved: March 14, 2024 | Published: March 15, 2024
How to cite this article: Al-Anazi KA, Alsaffar WA, Aljishi FK, Kanfer S, Kalogiannidis P, et al. The Outcome of Patients with Leukemia Presenting with Hyperleukocytosis Requiring Leukapheresis. The Experience of King Fahad Specialist Hospital in Dammam, Saudi Arabia. J Hematol Clin Res. 2024; 8: 008-016.
DOI: 10.29328/journal.jhcr.1001028
Copyright License: © 2024 Al-Anazi KA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Hyperleukocytosis; Leukostasis; Leukapheresis; Acute leukemia; Chronic myeloid leukemia; Hematopoietic stem cell transplantation

The Outcome of Patients with Leukemia Presenting with Hyperleukocytosis Requiring Leukapheresis. The Experience of King Fahad Specialist Hospital in Dammam, Saudi Arabia
Khalid Ahmed Al-Anazi1*, Alsaffar WA1, Aljishi FK1, Kanfer S1, Kalogiannidis P1, Alenazi W1, Alshammasi Z1, Albahrani A2, Abduljalil O1, Mutahar E1, Alwakeel AM1, Apostolidis I1, Darweesh M1, Almokhtar N1, Abdulbaqi M1, Albanyan O1, Alshaibani Z1, Raslan H3, Aldayel A3, Alrabeh R3, Dridi W4, Alharbi S1, Alshami A1, Ayyad A1, Alsomali Z1, Albatran M1, Alhowaish K5, Alblowe BA1, Alamri A2 and Abu Rahma F1
1Department of Hematology and Hematopoietic Stem Cell Transplantation, Oncology Center, King Fahad Specialist Hospital, P.O. Box: 15215, Dammam 31444, Saudi Arabia
2Apheresis and Blood Bank, Department of Pathology and Central Laboratory, King Fahad Specialist Hospital, P.O. Box: 15215, Dammam 31444, Saudi Arabia
3Hematopathology and Flowcytometry, Department of Pathology and Central Laboratory, King Fahad Specialist Hospital, P.O. Box: 15215, Dammam 31444, Saudi Arabia
4Cytogenetics, Department of Pathology and Central Laboratory, King Fahad Specialist Hospital, P.O. Box: 15215, Dammam 31444, Saudi Arabia
5Clinical Pharmacy, Department of Pharmacy, King Fahad Specialist Hospital, P.O. Box: 15215, Dammam 31444, Saudi Arabia
*Address for Correspondence: Dr. Khalid Ahmed Al-Anazi, Consultant Hemato-Oncologist, Department of Hematology and Hematopoietic Stem Cell Transplantation, Oncology Center, King Fahad Specialist Hospital, P.O. Box: 15215, Dammam 31444, Saudi Arabia. Email: [email protected]
Background: Patients with acute and chronic leukemia presenting with hyperleukocytosis are at risk of developing leukostasis which has serious and life-threatening complications. Leukapheresis is usually performed to reduce the complications of leukostasis in patients presenting with hyperleukocytosis and clinical manifestations compatible with leukostasis.
Methods and materials: A retrospective study of patients with acute and chronic leukemia who received leukapheresis for hyperleukocytosis between the 1st of January 2013 and the 31st of December 2023 at King Fahad Specialist Hospital (KFSH) in Dammam, Saudi Arabia was performed.
Results: Over a period of 11 years, a total of 50 patients with acute and chronic leukemia presenting with hyperleukocytosis and clinical manifestations of leukostasis; 32 patients with acute leukemia (AL) and 18 patients with chronic myeloid leukemia (CML); received leukapheresis at our institution. Among the 32 patients with AL who received leukapheresis, 24 patients (75%) had acute myeloid leukemia (AML), 7 patients (21.88%) had acute lymphoblastic leukemia (ALL) and 1 patient (3.13%) had bilineage acute leukemia (BAL). At presentation of their AL: 3 patients (9.38%) had fever, 9 patients (28.13%) had infections, 4 patients (12.5%) had palpable spleen or liver, 6 patients (18.75%) had palpable external lymph nodes, and 9 patients (28.13%) had extramedullary disease (EMD). After receiving induction and consolidation cycles of chemotherapy, 11 patients (34.38%) of AL patients received allogeneic hematopoietic stem cell transplantation (HSCT). At the end of the follow-up, 17 patients (53.1%) with AL were alive while 15 patients (46.9%) were dead. The 8-year overall survival (OS) for all patients with AL subjected to leukapheresis was 47%. The 5 years OS for patients with AL who subsequently received HSCT and those who did not receive allogeneic HSCT were 70% and 40% respectively. The mean white blood cell (WBC) count of CML patients subjected to leukapheresis was 465.5 × 109/L, 11 patients (61.11%) had clear signs of leukostasis, and 8 patients (44.44%) had splenomegaly at presentation. Regarding the disease stage at presentation, 14 CML patients (77.78%) had chronic phase (CP), 2 patients (11.11%) had accelerated phase (AP) and 2 patients (11.11%) had blast phase (BP). Regarding the fate of CML patients at the end of the study were: 15 (83.33%) were alive, 1 (5.56%) dead, and 2 (11.11%) were unknown as they lost follow-up. However, the 10-year OS of patients with CML subjected to leukapheresis was 90%.
Conclusion: Patients with acute or chronic leukemia presenting with hyperleukocytosis and either ongoing or impending leukostasis should have urgent cytoreductive chemotherapy and leukapheresis to prevent life-threatening complications. Although the outcome of AL patients presenting with leukostasis is generally poor, prompt cytoreductive therapy and leukapheresis, followed by induction chemotherapy and allogeneic HSCT may improve the outcome. Also, urgent cytoreduction including leukapheresis improves the outcome of patients with CML presenting with hyperleukocytosis and leukostasis.
AML, ALL, and CML are heterogeneous diseases that carry widely variable prognoses which depend on disease status and patient characteristics [1]. Nowadays, the standard first-line therapy is the combination of gemtuzumab ozogamicin or midostaurin with intensive chemotherapy for fit AML patients, and the combination of azacitidine and venetoclax for unfit patients [2]. The recent major advances in the management of AML include: new insights on the molecular pathogenesis, risk classification, technological progress in genomic diagnostics, use of measurable residual disease (MRD), and introduction of several novel therapies including isocitrate dehydrogenase (IDH) inhibitors; B cell leukemia/lymphoma-2 (BCL2) inhibitors; FMS-like tyrosine kinase 3 (FLT3) inhibitors; gemtuzumab ozogamicin; magrolimab; and menin inhibitors [3,4].
The recent incorporation of pediatric-inspired chemo-therapeutic protocols in the treatment of adult patients with ALL resulted in improvement in the prognosis and decrease in the use of allogeneic HSCT [5]. The treatment of ALL has been revolutionized with the introduction of the following novel therapies: tyrosine kinase inhibitors (TKIs) targeting BCR/ABL1, monoclonal antibodies targeting CD20 such as rituximab, antibody-drug conjugates targeting CD22 including inotuzumab ozogamicin, bispecific antibodies such as blinatumomab, and CD19 chimeric antigen receptor (CAR) T-cell therapy [5-7]. Allogeneic HSCT is indicated in selected ALL patients as it offers a survival benefit [8]. Reduced intensity/non-myeloablative conditioning regimens have achieved outcomes comparable to total body irradiation (TBI)-based myeloablative conditioning (MAC) in older patients with ALL having positive Philadelphia chromosome in first complete hematological remission (CHR1) [9]. Also, the use of CD19 CAR- T cells have increased the response rate in patients with refractory or relapsed B-cell ALL [10].
The following TKIs have been introduced into the treatment of CML in the chronic phase (CML-CP): imatinib, dasatinib, bosutinib, and nilotinib [11,12]. Some CML patients progress to AP and BP which have a relatively poor prognosis [11]. The combination of ponatinib with intensive chemotherapy followed by allogeneic HSCT can achieve long-term survival in some transformed BP patients [11,13]. Therapeutic regimens including venetoclax in myeloid BP or inotuzumab ozogamicin or blinatumomab in lymphoid BP might result in deeper responses and bridge patients to allogeneic HSCT once a second CP is achieved [11].
The success of allogeneic HSCT, which is potentially curative for patients with AL, is limited by transplant-related mortality (TRM) [14,15]. The risk factors for early TRM include age, time from diagnosis to transplantation, number of prior transplantations, graft source, and prior iron chelation therapy [15]. In patients with leukemia, treatment decisions, and prognosis depend on the patient’s disease status and require accurate assessment of MRD [1]. Achievement of MRD negativity is associated with superior disease-free survival (DFS) and OS in patients with AML and is essential in pediatric and adult ALL patients [16,17]. Also, a large retrospective study showed that the presence of MRD with the persistence of FLT3-ITD or NPM1 variants in patients with AML prior to HSCT was associated with increased relapse rate and worse survival [18].
A retrospective study of patients with acute and chronic leukemia who presented with hyperleukocytosis and leukostasis requiring leukapheresis between the 1st of January 2013 and the 31st of December 2023 at KFSH in Dammam, Saudi Arabia was performed. The medical records, and the clinical data as well as the laboratory data of all patients with leukemia (AML, ALL, and CML) who received leukapheresis at KFSH in Dammam, Saudi Arabia during the time period specified above were retrieved for analysis. During the study period, several patients with chronic lymphocytic leukemia (CLL) presented with hyperleukocytosis but none of them developed leukostasis requiring leukapheresis.
For AL patients presenting with hyperleukocytosis and leukostasis, the initial management consisted of cytoreductive chemotherapy, with corticosteroids for ALL patients and hydroxyurea and/or cytarabine for AML patients, in addition to leukapheresis followed by induction chemotherapy. For AML patients, the induction therapy consisted of daunorubicin or idarubicin plus cytarabine (3+7) regimen and mitoxantrone, etoposide, and cytarabine (MEC) salvage for patients with refractoriness to the first line therapy. For ALL patients, the induction therapy consisted of one of 3 protocols: Children’s Cancer Group (CCG-1961); cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride (adriamycin), methotrexate (Hyper-CVAD); and Berlin-Frankfurt-Münster protocol (BFM), while salvaging chemotherapy in the form of fludarabine, cytarabine, and idarubicin with or without granulocyte colony-stimulating factor (G-CSF) [FLAG-IDA and FLA-IDA] or Hyper-CVAD (for those who did not receive it as induction) was given for patients with refractory ALL.
The consolidation therapy was in the form of high-dose cytosine arabinoside (HiDAC) for standard-risk (SR) AML patients and in the form of consolidation followed by maintenance chemotherapy as per CCG-1961, Hyper-CVAD and BFM protocols of chemotherapy for SR-ALL patients. However, all high-risk (HR) AL patients were consolidated with allogeneic HSCT if they were transplant-eligible. Additional therapy was given with FLT3 inhibitors, rituximab, and TKIs for FLT3 mutations, CD 20 positivity and Philadelphia chromosome respectively.
For patients with CML, TKIs were commenced following cytoreductive therapy and leukapheresis and after confirming the diagnosis of CML with positive BCR/ABL transcript. Disease evaluation using clinical as well as laboratory parameters including BCR/ABL transcript was performed at regular intervals; initially monthly then 3 monthly and ultimately every 6 months throughout their follow-up. For those patients developing adverse effects related to one form of TKI therapy or failing to achieve the expected milestones, shifting to another line of TKI therapy was indicated.
In patients with leukemia presenting with hyper-leukocytosis, established leukostasis was defined as having one or more of the following clinical manifestations: severe mental confusion, severe shortness of breath, and acute renal failure; while impending leukostasis was defined as having mild to moderate manifestations of leukostasis such as: fatigue, disorientation or mild mental confusion, chest tightness or mild shortness of breath, and acute renal dysfunction. Leukapheresis was usually commenced within a few hours of the arrival of patients to the emergency room after obtaining the results of complete blood count and peripheral blood film and inserting the appropriate central venous catheter in patients with AL or CML presenting with hyperleukocytosis and either ongoing or impending leukostasis.
Statistical analysis
The SSPS version 22 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. The Kaplan-Meier method with a log-rank test was used to estimate the survival rates and to identify risk factors that influenced the treatment outcome. OS was defined as the duration from the day of diagnosis until death or the date of the last follow-up for live patients with AML, ALL, and CML.
During the study period of 11 years, a total of 50 patients with acute and chronic leukemia; 32 patients with AL, and 18 patients with CML; presenting with hyperleukocytosis and either ongoing or impending leukostasis received leukapheresis at our institution.
Regarding the 32 patients with AL who received leukapheresis, there were 23 males and 9 females. Their ages ranged between 17 and 72 years with a mean age of 40.56 years. Twenty-four patients (75%) had AML (1 M0, 6 M1, 2 M2, 5 M4, 10 M5), 7 patients (21.9%) had ALL (4 B-cell type and 3 T-cell type) and only 1 patient (3.1%) had BAL. The mean WBC count at diagnosis was 376.9 × 109/L. Seventeen patients (53.1%) with AL (15 AML and 2 ALL) had established clinical and laboratory manifestations of leukostasis while 15 patients (46.9%) with AL (9 AML, 5 ALL, and 1 BAL) presented with hyperleukocytosis and impending leukostasis. The sites of leukostasis were: respiratory system (RS) in 9 patients; central nervous system (CNS) in 6 patients; both RS and CNS in 1 patient; and RS, CNS, and kidneys in 1 patient. The number of sessions of leukapheresis ranged between 1 and 4 with a mean of 2.5 sessions per patient. At the presentation of their AL: 3 patients (9.38%) had fever alone, 9 patients (28.13%) had infections, 4 patients (12.5%) had palpable spleen or liver, 6 patients (4 AML and 2 ALL) patients (18.75%) had palpable external lymph nodes, and 9 (6 AML and 3 ALL) patients (28.13%) had EMD (Table 1). The involved EMD sites included: CNS, paranasal sinuses, retina, pleural cavity, lungs, kidneys, and skin. Six AML patients (3 M5, 2 M4, and 1 M1) and 3 patients with ALL (2 B-cell type and 1 T-cell type) had EMD at diagnosis. The number of EMD sites was as follows: 1 site in 7 patients (5 AML, and 2 ALL); 3 sites in 1 patient with T-cell ALL; and 4 sites in 1 patient with AML-M4 subtype. A total of 19 patients with AL had adverse cytogenetic abnormalities at presentation (Table 1). The adverse cytogenetic abnormalities and molecular mutations were as follows: FLT3 mutations in 10 patients [3 of them had additional nucleophosmin 1 (NPM1) mutation], mixed bilineage leukemia (MLL) mutation in 2 patients, Philadelphia chromosome in 3 patients, and complex cytogenetics in 2 patients. Eight patients with adverse cytogenetics received allografts while 11 other AL patients with adverse cytogenetics did not receive allogeneic HSCT (Table 1).
| Table 1: Patients with Acute Leukemia Presenting with Hyperleukocytosis Subjected to Leukapheresis. | ||||
| Features and Abnormalities | Patients Subjected to HSCT (11 patients) | Patients Not Subjected to HSCT (21 patients) | ||
| Number | Percentage | Number | Percentage | |
| Fever and Infections at Presentation | 6 | 54.55 | 7 | 33.33 |
| Extramedullary Disease at Diagnosis | 3 | 27.27 | 6 | 28.57 |
| External Lymphadenopathy at Diagnosis | 0 | 0.0 | 6 | 28.57 |
| Abdominal Organomegaly at Diagnosis | 2 | 18.18 | 1 | 4.76 |
| Adverse Cytogenetics at Diagnosis | 8 | 72.73 | 11 | 52.38 |
| Status at the End of the Study (Alive or Dead) |
Alive: 8 Dead: 3 |
72.73 27.27 |
Alive: 9 Dead: 12 |
42.86 57.14 |
| HSCT: Hematopoietic Stem Cell Transplantation | ||||
Following induction therapy, 18 patients of AL (56.25%) achieved CHR with less than 5% bone marrow (BM) blasts, 10 patients (31.25%) achieved partial remission (PR) with 5% - 15% BM blasts, 3 patients (9.38%) had refractory disease, while no evaluation was done for 1 patient who died of sepsis before reaching day 28 of induction therapy. However, 8 AL patients developed infectious complications and sepsis and 3 of these patients needed intensive care unit (ICU) admission for inotropes or mechanical ventilation during the first cycle of chemotherapy. After the second cycle of chemotherapy for AL patients, 5 patients developed febrile neutropenia and 2 of them developed septic shock. All 10 patients who achieved PR after the first cycle of chemotherapy had CHR after the second cycle of chemotherapy [8 with negative MRD and 2 with positive MRD].
After receiving induction and consolidation cycles of chemotherapy, 11 patients (34.38%) with AL (7 AML, 3 ALL, and 1 BAL) subsequently received allogeneic HSCT (Tables 1,2). The conditioning therapy was myeloablative in 8 patients and reduced intensity in 3 patients. Peripheral blood was the source of stem cells in all patients subjected to HSCT. Regarding the disease status before HSCT, 8 patients were in the first CHR, 2 patients were in the second CHR, and 1 patient received sequential therapy as he had refractory disease. Pre-transplant MRD was negative in 8 recipients of HSCT. Allogeneic HSCT was successful in 9 recipients and unsuccessful in 2 transplant recipients including one patient who received sequential therapy. The complications encountered in allograft recipients were as follows: mucositis in 7 patients, hemorrhagic cystitis in 2 patients, acute graft versus host disease (GVHD) in 6 patients (4 gastrointestinal tract and 2 skin), chronic GVHD in 4 patients, and various infectious complications in 10 patients: 5 bacterial, 4 cytomegalovirus and 1 fungal infection (Table 2). At the end of the follow-up, 17 patients (53.1%) with AL were alive while 15 patients (46.9%) were dead. The 8-year OS for all patients with AL subjected to leukapheresis was 47% (Figure 1). The 5 years OS for patients with AL who subsequently received HSCT and those who did not receive allogeneic HSCT were 70% and 40% respectively (Figure 2). At the end of the study, 72.73% of patients with AL subjected to HSCT were alive while 42.86% of AL patients not subjected to HSCT were alive (Table 1).
| Table 2: Data of the patients with acute leukemia subjected to hematopoietic stem cell transplantation (HSCT). | ||
| Disease and HSCT Features | Details | Specific Details |
| Primary disease | Acute myeloid leukemia (AML): 8 (72.73%) Acute lymphoblastic leukemia (ALL): 2 (18.18%) Bilineage acute leukemia: 1 (9.09%) |
5 AML-M5; 1 AML-M4; 1 AML-M1; 1 AML-M0; 2 B-ALL; 1 T-ALL |
| Type of HSCT | Sibling allogeneic: 9, Haploidentical HSCT: 2 | Sibling donor: 81.82% Haploidentical donor: 18.18% |
| Conditioning Therapy | Myeloablative: 8, Reduced intensity: 3 | Myeloablative conditioning: 72.73% Reduced intensity conditioning: 27.27% |
| Disease Status before HSCT | First complete hematological remission (CHR1): 8 (72.73%) Second complete hematological remission (CHR2): 2 (18.18%) Refractory disease: 1 (9.09%) |
CHR1 with no measurable residual disease (MRD): 7 CHR1 with MRD: 1 CHR2 with no MRD: 2 |
| Post-HSCT Complications | Acute graft versus host disease (GVHD): 6 (54.55%) Chronic GVHD: 4 (36.36%) Mucositis; grades: I to III: 7 (40.5%) Hemorrhagic cystitis: 2 (18.18%) Vono-occlusive disease of the liver: 0 Infections: 10 (90.9%) |
Acute GVHD: 4 gastrointestinal tract; 2 skin Chronic GVHD: all more than 1 organ Infections: Bacterial: 5 Cytomegalovirus: 4 Fungal: 1 |
| Outcome at end of follow-up | Alive: 8 (72.73%) Deceased: 3 (22.27%) |
Causes of death: Disease progression: 1 Sepsis and infections: 2 |
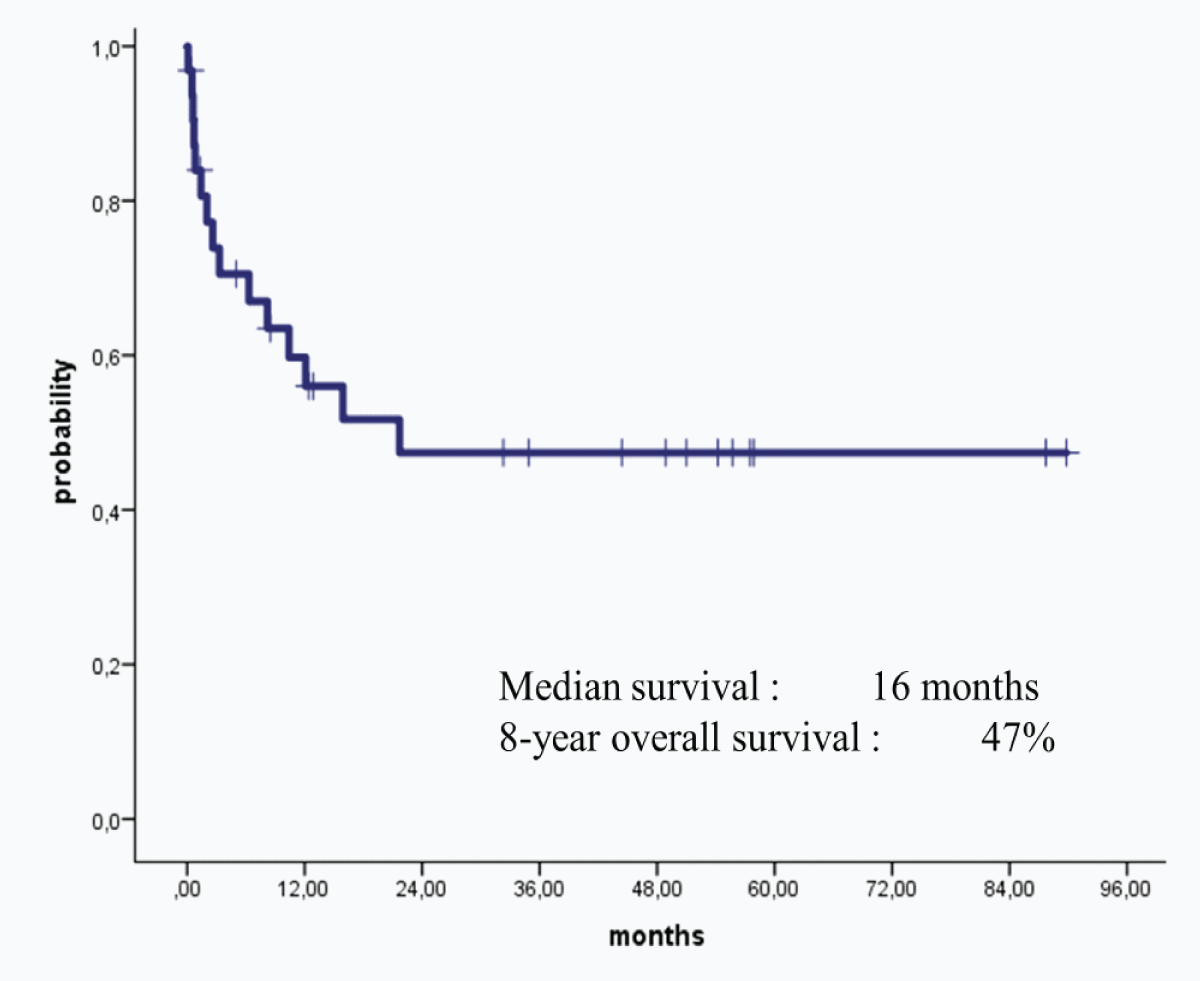
Figure 1: Overall Survival for Acute leukemia patients.
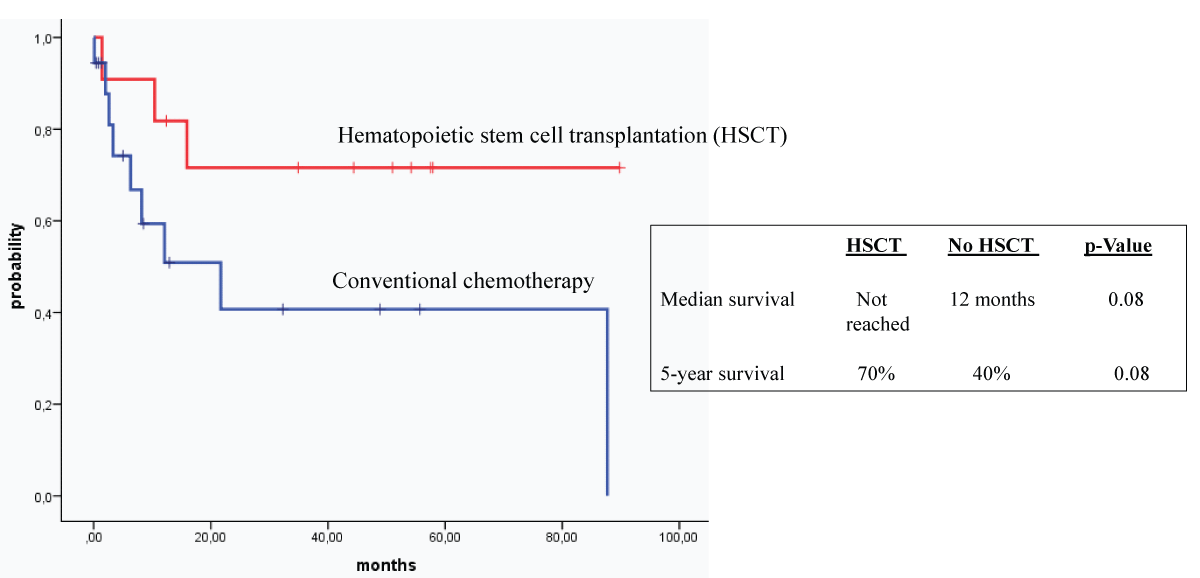
Figure 2: Overall survival for patients presented with leukocytosis according to type of consolidation
Regarding the 18 patients with CML who received leukapheresis, 12 were males and 6 were females and their ages ranged between 19 and 70 years with a mean age of 36.6 years. All CML patients presented with very high WBC counts with a mean WBC count of 465.5 × 109/L, 16 patients (88.89%) presented with anemia, while only 3 patients (16.67%) had thrombocytopenia at presentation. Eleven patients (61.11%) of CML patients had clinical manifestations of leukostasis with 5 in the brain, 3 in the lung, and 3 in other sites including kidneys, while 7 patients had hyperleukocytosis with impending leukostasis (Table 3). The number of sessions of leukapheresis ranged between 1 and 5 with a mean of 2.7 sessions per patient. Sixteen CML patients required hydroxyurea alone as cytoreductive chemotherapy while 2 patients required hydroxyurea plus steroids or hydroxyurea plus intravenous cytosine arabinoside for lymphoid and myeloid BP respectively. All CML patients had positive Philadelphia chromosomes with t 9,22 confirmed in all cases. P210 of BCR/ABL transcript was confirmed in 16 patients with CP and 1 patient with myeloid BP of CML, while p190 of BCR/ABL was positive in 1 patient with lymphoid BP. Regarding the disease stage at presentation, 14 CML patients (77.78%) had CP, 2 patients (11.11%) had AP and 2 patients (11.11%) had BP. Three patients (16.67%) had fever at diagnosis, 8 patients (44.44%) had splenomegaly, and only 1 patient (5.56%) had EMD at presentation (Table 3). The first line TKI therapy was imatinib in 10 patients, dasatinib in 5 patients, and nilotinib in 2 patients while interferon was given to 1 CML patient. The second line of TKI therapy was needed in 10 out of 18 patients. TKI therapies were complicated by: cytopenias in 6 patients, pleural effusions in 3 patients, and skin eruptions in 1 patient. None of the patients with CML-CP required allogeneic HSCT, while the 2 patients with BP had successful allografts. The levels of BCR/ABL transcripts at the end of follow-up at our institution were as follows: < 0.1% in 7 patients, 0.1% - 10% in 2 patients, > 10% in 6 patients, 100% in 1 patient, and unknown in 2 patients who moved to have treatment at other institutions (Table 3). Regarding the fate of CML patients at the end of the study were: 15 (83.33%) alive, 1 (5.56%) dead, and 2 (11.11%) unknown as they lost follow-up (Table 3). The 10-year OS of patients with CML subjected to leukapheresis was 90% (Figure 3).
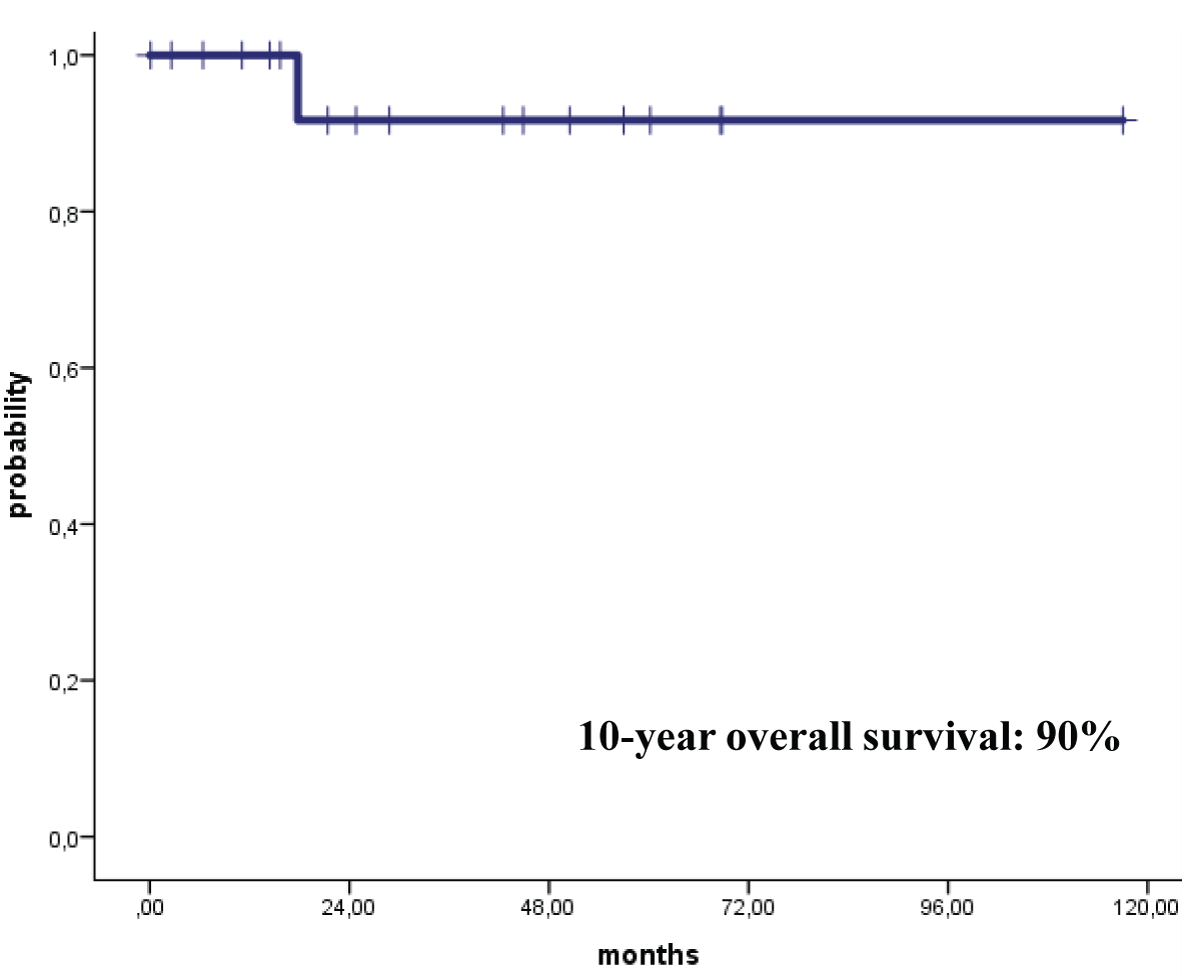
Figure 3: Overall Survival for CML Patients.
| Table 3: Data of Patients with Chronic Myeloid Leukemia Presenting with Hyperleukocytosis Subjected to Leukapheresis. | ||
| Features and Abnormalities | Numbers | Percentages and Details |
| Stage of Disease at Diagnosis | Chronic Phase (CP): 14 Accelerated Phase (AP): 2 Blast Phase (BP): 2 |
CP: 77.78% AP: 11.11% BP: 11.11% |
| Blood Counts at Presentation | High WBC count in all patients; Mean WBC count: 465.5 Hemoglobin: Normal in 2 patients; Low in 16 patients Platelet (PLT) Count: Normal in 15 patients; Low in 3 patients |
Very high WBC: 100% Anemia: 88.89% Low PLTs: 16.67% |
| Clinical Manifestations at Presentation | Splenomegaly: 8; Fever: 3 External lymphadenopathy (LAP): 2 [in patient with lymphoid BP] Extramedullary disease (EMD): 1 [the patient had CP] Fatigue:1; Weight loss: 1 |
Splenomegaly: 44.44%; Fever: 16.67% External LAP: 11.11% EMD: 5.56% Fatigue: 5.56%; Weigh loss: 5.56% |
| Established or Ongoing Lekostasis at Diagnosis | Present in 11 patients Sites: brain: 5; Lung: 3; Other sites including kidneys: 3 |
Leukostais present in 61.11% Brain: 27.78%; Lungs: 16.67% Other sites: 16.67% |
| Additional Cytoreductive Chemotherapy | Needed in all patients Hydroxyurea (HU): 16 patients HU + Corticosteroids: 1 patient HU + intravenous cytarabine: 1 patient |
100% of patients needed cytoreduction with leukapheresis. HU alone: 88.89% HU + Other agents: 11.11% |
| Cytogenetic Abnormalities at Presentation | All patients had Philadelphia (Ph) chromosome (t 9,22) BCR/ABL p210: 17 patients [16 CP and 1 Myeloid BCC] BCR/ABL p190: 1 patient with lymphoid BCC t 1,20 in 1 patient with CP |
+ Ph chromosome: 100% BCR/ABL p210: 94.44% BCR/ABL p190: 5,56% t 1,20: 5.56% |
| First-line Tyrosine Kinase Inhibitor (TKI) Therapy | Imatinib: 10 Dasatinib: 5 Nilotinib: 2 |
Imatinib: 55.56% Dasatinib: 27.78% Nilotinib: 11.11% |
| Level of BCR/ABL Transcript at Last Follow-up | < 0.1%: 7 patients; 0.1-10%: 2 patients > 10%: 6 patients; 100%: 1 patient Not Done: 2 patients |
< 0.1%: 38.89%; 0.1% -10%: 11.11% > 10%: 33.33%; 100%: 5.56% Not Done: 11.11% |
| Status at the End of the Study (Alive or Dead) |
Alive: 15 patients Deceased: 1 patient Unknown: 2 (moved to other institutions) |
Alive: 83.33% Deceased: 5.56% Unknown: 11.11% |
| HSCT: Hematopoietic Stem Cell Transplantation; WBC: White Blood Cell | ||
Hyperleukocytosis, which is caused by leukemic cell proliferation, is a laboratory abnormality that is commonly defined by a WBC count > 100 × 109 / L [19-22]. The risk factors for hyperleukocytosis include (1) certain hematologic malignancies including (a) AML, particularly myelomonocytic or monocytic/monoblastic morphology and micro granular variant of acute promyelocytic leukemia (APL); (b) ALL, particularly T-cell subtype; (c) CLL; (d) CML, particularly in AP or BP; (2) specific cytogenetic abnormalities including 11q23 rearrangements, inversion 16, FLT3-internal tandem duplication (ITD), and presence of the Philadelphia chromosome; (3) male gender; (4) younger age groups; and (5) huge splenomegaly [19,22,23]. Two main pathogenetic factors are responsible for the development of hyperleukocytosis: (1) rapid blast proliferation leading to a high leukemic tumor burden; and (2) disruption in normal hematopoietic cell adhesion leading to a reduced affinity to the BM [19]. In our study, hyperleukocytosis was encountered in 24 patients (48%) with AML, 18 patients (36%) with CML, 7 patients (14%) with ALL, and 1 patient (2%) with BAL. In patients with AL, 19 patients (59.4%) had adverse cytogenetic abnormalities including FLT3 mutation, MLL, Philadelphia chromosome, and complex cytogenetics. Splenomegaly was encountered in 11 patients (22%), 8 patients with CML and 3 patients with AL. The mean WBC count at diagnosis was 376.9 × 109/L and 465.5 × 109/L for patients with AL and CML respectively.
The most common clinical features of hyperleukocytosis include (1) neurological manifestations such as headache, confusion, lethargy, dizziness, blurred vision, ataxia, papilledema, retinal hemorrhage and intracranial hemorrhage; (2) respiratory features including tachypnea, dyspnea, hypoxia, pulmonary infiltrates and respiratory failure; (3) renal manifestations such as acute renal failure; (4) metabolic abnormalities as part of tumor lysis syndrome (TLS); (5) disseminated intravascular coagulation (DIC) and coagulopathy; and (5) involvement of other systems such as congestive heart failure, myocardial infarction, peripheral vascular occlusion, priapism, and multisystem failure [22,24,25]. The main complications of hyperleukocytosis include (1) leukostasis; (2) DIC; and (3) TLS [19,22,26]. However, the complications of leukostasis include (1) hyperviscosity syndrome; (2) vascular occlusion causing intracranial hemorrhages and respiratory failure; and (3) perivascular leukemic infiltrates [27]. The risk of pulmonary leukostasis, which is one of the most common life-threatening complications in patients with hyperleukocytosis, is higher in myeloid leukemia with WBC counts greater than 100×109/L [28]. In the lung, the clinical presentation simulates infections and hemorrhagic complications of acute leukemia [29]. The only diagnostic test to confirm the presence of pulmonary leukostasis is lung biopsy. Hence, a high level of clinical suspicion should be maintained and early cytoreduction with leukapheresis and chemotherapy should be initiated [30]. Being a medical emergency, early recognition of leukostasis and initiation of therapy prevents mortality [29]. Definitive treatment of pulmonary leukostasis is still controversial. However, early detection and treatment by cytoreduction may improve outcomes [28]. In our study, 28 patients (56%) had ongoing leukostasis (12 in lungs, 11 in CNS, and 5 in other organs) while 22 patients (44%) had impending leukostasis. All our 50 leukemia patients had leukapheresis and the mean numbers of leukapheresis sessions performed per patient were 2.5 for AL and 2.7 for CML patients.
Management of hyperleukocytosis consists of: (1) treatment of leukostasis that includes cytoreduction with leukapheresis, induction chemotherapy, hydroxyurea, and targeted agents against endothelial adhesion; (2) treatment of TLS with supportive and prophylactic treatment with intravenous (IV) fluids, allopurinol and rasburicase; and (3) treatment of DIC that includes supportive and prophylactic treatment with (a) transfusion of platelets, fibrinogen, fresh frozen plasma, and packed red blood cells, and (b) administration of recombinant thrombomodulin, recombinant activated factor VIIa, and antithrombin or activated protein C [19,22,26]. A retrospective study that included 47 pediatric patients having AL and presenting with hyperleukocytosis showed that repeated small-volume exchange transfusion is effective and safe [31]. Exchange transfusion or leukapheresis together with conservative management and specific oncological therapy may contribute to rapid leukocyte reduction with acceptable risk [32]. In our study, all patients received cytoreductive chemotherapy in addition to leukapheresis and supportive measures including allopurinol, and IV fluids for hydration and correction of electrolytic disturbances. The initial cytoreductive chemotherapy was in the form of corticosteroids for ALL patients, hydroxyurea with or without cytarabine for AML patients, and hydroxyurea alone for CML patients. However, a few of our patients whose clinical condition was critical received their leukapheresis and initial therapies in the ICU.
Leukapheresis is performed using apheresis equipment to separate leukocytes from peripheral blood while at the same time, it returns autologous plasma, platelets, and erythrocytes to the patient. It is applied clinically for the treatment of hyperleukocytosis by rapidly removing excessive leukocytes and correcting metabolic abnormalities in addition to alleviating the symptoms of leukostasis [33]. Several studies have shown that the procedure is generally safe and well-tolerated [33-35]. In patients with leukemia presenting with hyperleukocytosis, studies have shown that although leukapheresis can rapidly reduce the elevated WBC count and result in symptomatic relief, it did not improve short-term or long-term survival [27,36-38]. Additionally, 3 systematic reviews and meta-analyses that included 45 studies in patients with leukemia presenting with hyperleukocytosis confirmed that the use of leukapheresis had no effect on short-term or long-term survival [26,39,40]. Hence, leukapheresis should be offered to patients having clinical manifestations of leukostasis but routine performance of prophylactic leukapheresis is not recommended [26,37]. However, several other studies have shown the effectiveness of leukapheresis in reducing the high WBC counts in children and adults; reducing early mortality due to hyperleukocytosis; and improving OS of patients particularly when leukapheresis is combined with cytoreductive therapy using drugs such as hydroxyurea and cytosine arabinoside [33-35,41-45]. Recently, leukapheresis has become one of the most effective adjuvant therapies in treating hyperleukocytosis and studies have shown the efficacy of leukapheresis even when used prophylactically in preventing the evolution of complications such as leukostasis and in reversing the negative impact of high leukemia burden achievement of disease remission later on [33,41,42,45]. Early and sudden deaths have been reported not only in patients with AL but also in patients with CML presenting with hyperleukocytosis and leukostasis in the absence of prompt leukapheresis [46-52]. In our study, no adverse effects or deaths were encountered due to leukapheresis per se. Despite having HR disease features in the majority of patients and encountering few patients with critical clinical conditions at diagnosis, only 1 early death before day 28 of induction therapy for AL was encountered and the patient died in ICU due to complications of AL and its therapy.
Several studies in pediatric and adult patients with AL have shown that hyperleukocytosis is associated with inferior OS due to to evolution of major complications of leukostasis, TLS, and DIC [25,33,36,41,43]. In patients with AML, hyperleukocytosis is an independent poor prognostic factor irrespective of cytogenetics and mutation status as it is associated with increased relapse rate, decreased leukemia-free survival, and inferior OS [53,54]. However, allogeneic HSCT in patients with AML can significantly improve the poor outcome of hyperleukocytosis [53-55]. The long-term outcomes of our leukemia patients subjected to leukapheresis were as follows: the 8-year OS for patients with AL patients was 47% while the 10-year OS for patients with CML was 90%. However, subgroup analysis showed that receiving allogeneic HSCT made a large difference in the long-term survival in patients with AL subjected to leukapheresis as the 5 years OS for recipients of HSCT was 70% while that for patients who did not receive allografts was 40%.
Despite including a relatively large number of patients in our study and that the study extended over 11 years, we acknowledge that retrospective studies have their own limitations.
Patients with AL and CML presenting with hyper-leukocytosis should be regarded as HR patients. Consequently, Leukapheresis should be urgently performed in patients having clinical manifestations consistent with either ongoing or impending leukostasis and surviving patients with AL should be offered allogeneic HSCT after control of their disease. Adding cytoreductive chemotherapy to the initial therapy and incorporating novel therapies later on during the course of the disease is essential to reduce or prevent the complications of leukostasis and to improve not only the short-term but also the long-term outcome of patients with leukemia presenting with hyperleukocytosis. It is difficult to perform prospective multicentre and randomized clinical trials in patients with acute and chronic leukemia presenting with leukostasis to determine the efficacy of leukapheresis.
Authors’ contributions
All authors participated in the management of the patients included in the study. Also, all authors read and approved the final form of the manuscript.
The authors are grateful to all medical, nursing, and technical staff at KFSH in Dammam, Saudi Arabia who participated in the management of the patients included in this retrospective study.
- Dekker SE, Rea D, Cayuela JM, Arnhardt I, Leonard J, Heuser M. Using Measurable Residual Disease to Optimize Management of AML, ALL, and Chronic Myeloid Leukemia. Am Soc Clin Oncol Educ Book. 2023 Jun;43:e390010. doi: 10.1200/EDBK_390010. PMID: 37311155.
- Huerga-Domínguez S, Villar S, Prósper F, Alfonso-Piérola A. Updates on the Management of Acute Myeloid Leukemia. Cancers (Basel). 2022 Sep 29;14(19):4756. doi: 10.3390/cancers14194756. PMID: 36230677; PMCID: PMC9563665.
- Döhner H, Wei AH, Appelbaum FR, Craddock C, DiNardo CD, Dombret H, Ebert BL, Fenaux P, Godley LA, Hasserjian RP, Larson RA, Levine RL, Miyazaki Y, Niederwieser D, Ossenkoppele G, Röllig C, Sierra J, Stein EM, Tallman MS, Tien HF, Wang J, Wierzbowska A, Löwenberg B. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022 Sep 22;140(12):1345-1377. doi: 10.1182/blood.2022016867. PMID: 35797463.
- Kayser S, Levis MJ. The clinical impact of the molecular landscape of acute myeloid leukemia. Haematologica. 2023 Feb 1;108(2):308-320. doi: 10.3324/haematol.2022.280801. PMID: 36722402; PMCID: PMC9890016.
- Rabian F, Boissel N. LAL chez l’adulte : apport et limite de la prise en charge pédiatrique [ALL in adult patients: Contribution and limits of pediatric management]. Bull Cancer. 2021 Feb;108(2):187-197. French. doi: 10.1016/j.bulcan.2020.07.008. Epub 2020 Sep 24. PMID: 32981690.
- Hoelzer D, Bassan R, Boissel N, Roddie C, Ribera JM, Jerkeman M; ESMO Guidelines Committee. Electronic address: [email protected]. ESMO Clinical Practice Guideline interim update on the use of targeted therapy in acute lymphoblastic leukaemia. Ann Oncol. 2024 Jan;35(1):15-28. doi: 10.1016/j.annonc.2023.09.3112. Epub 2023 Oct 11. PMID: 37832649.
- Samra B, Jabbour E, Ravandi F, Kantarjian H, Short NJ. Evolving therapy of adult acute lymphoblastic leukemia: state-of-the-art treatment and future directions. J Hematol Oncol. 2020 Jun 5;13(1):70. doi: 10.1186/s13045-020-00905-2. PMID: 32503572; PMCID: PMC7275444.
- DeFilipp Z, Advani AS, Bachanova V, Cassaday RD, Deangelo DJ, Kebriaei P, Rowe JM, Seftel MD, Stock W, Tallman MS, Fanning S, Inamoto Y, Kansagra A, Johnston L, Nagler A, Sauter CS, Savani BN, Perales MA, Carpenter PA, Larson RA, Weisdorf D. Hematopoietic Cell Transplantation in the Treatment of Adult Acute Lymphoblastic Leukemia: Updated 2019 Evidence-Based Review from the American Society for Transplantation and Cellular Therapy. Biol Blood Marrow Transplant. 2019 Nov;25(11):2113-2123. doi: 10.1016/j.bbmt.2019.08.014. Epub 2019 Aug 22. PMID: 31446198.
- de Oliveira Fernandes Junior I, Arcuri LJ. Myeloablative or reduced-intensity/non-myeloablative hematopoietic cell transplantation for Philadelphia-positive acute lymphoblastic leukemia in adults older than 40 years old - a secondary analysis of a CIBMTR database. Ann Hematol. 2024 Feb;103(2):603-607. doi: 10.1007/s00277-023-05532-8. Epub 2023 Nov 9. PMID: 37940716.
- Pan J. Chimeric Antigen Receptor T Cell Therapy for Acute Leukemia. Blood Cell Ther. 2023 Nov 25;6(4):145-150. doi: 10.31547/bct-2023-028. PMID: 38149027; PMCID: PMC10749733.
- Senapati J, Jabbour E, Kantarjian H, Short NJ. Pathogenesis and management of accelerated and blast phases of chronic myeloid leukemia. Leukemia. 2023 Jan;37(1):5-17. doi: 10.1038/s41375-022-01736-5. Epub 2022 Oct 29. PMID: 36309558.
- Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2022 update on diagnosis, therapy, and monitoring. Am J Hematol. 2022 Sep;97(9):1236-1256. doi: 10.1002/ajh.26642. Epub 2022 Jul 6. PMID: 35751859.
- Jain P, Kantarjian HM, Ghorab A, Sasaki K, Jabbour EJ, Nogueras Gonzalez G, Kanagal-Shamanna R, Issa GC, Garcia-Manero G, Kc D, Dellasala S, Pierce S, Konopleva M, Wierda WG, Verstovsek S, Daver NG, Kadia TM, Borthakur G, O'Brien S, Estrov Z, Ravandi F, Cortes JE. Prognostic factors and survival outcomes in patients with chronic myeloid leukemia in blast phase in the tyrosine kinase inhibitor era: Cohort study of 477 patients. Cancer. 2017 Nov 15;123(22):4391-4402. doi: 10.1002/cncr.30864. Epub 2017 Jul 25. PMID: 28743165; PMCID: PMC5673547.
- Seftel MD, Pasic I, Parmar G, Bucher O, Allan DS, Bhella S, Hay KA, Ikuomola O, Musto G, Prica A, Richardson E, Truong TH, Paulson K. Hematopoietic Cell Transplantation Trends and Outcomes in Canada: A Registry-Based Cohort Study. Curr Oncol. 2023 Nov 17;30(11):9953-9967. doi: 10.3390/curroncol30110723. PMID: 37999143; PMCID: PMC10669983.
- Kong SG, Jeong S, Lee S, Jeong JY, Kim DJ, Lee HS. Early transplantation-related mortality after allogeneic hematopoietic cell transplantation in patients with acute leukemia. BMC Cancer. 2021 Feb 18;21(1):177. doi: 10.1186/s12885-021-07897-3. PMID: 33602150; PMCID: PMC7891151.
- Short NJ, Zhou S, Fu C, Berry DA, Walter RB, Freeman SD, Hourigan CS, Huang X, Nogueras Gonzalez G, Hwang H, Qi X, Kantarjian H, Ravandi F. Association of Measurable Residual Disease With Survival Outcomes in Patients With Acute Myeloid Leukemia: A Systematic Review and Meta-analysis. JAMA Oncol. 2020 Dec 1;6(12):1890-1899. doi: 10.1001/jamaoncol.2020.4600. PMID: 33030517; PMCID: PMC7545346.
- Berry DA, Zhou S, Higley H, Mukundan L, Fu S, Reaman GH, Wood BL, Kelloff GJ, Jessup JM, Radich JP. Association of Minimal Residual Disease With Clinical Outcome in Pediatric and Adult Acute Lymphoblastic Leukemia: A Meta-analysis. JAMA Oncol. 2017 Jul 13;3(7):e170580. doi: 10.1001/jamaoncol.2017.0580. Epub 2017 Jul 13. PMID: 28494052; PMCID: PMC5824235.
- Dillon LW, Gui G, Page KM, Ravindra N, Wong ZC, Andrew G, Mukherjee D, Zeger SL, El Chaer F, Spellman S, Howard A, Chen K, Auletta J, Devine SM, Jimenez Jimenez AM, De Lima MJG, Litzow MR, Kebriaei P, Saber W, Weisdorf DJ, Hourigan CS. DNA sequencing to detect residual disease in adults with acute myeloid leukemia prior to hematopoietic cell transplant. JAMA. 2023; 329(9): 745-755. doi: 10.1001/jama.2023.1363.
- Röllig C, Ehninger G. How I treat hyperleukocytosis in acute myeloid leukemia. Blood. 2015 May 21;125(21):3246-52. doi: 10.1182/blood-2014-10-551507. Epub 2015 Mar 16. PMID: 25778528.
- Gong J, Wu B, Guo T, Zhou S, He B, Peng X. Hyperleukocytosis: A report of five cases and review of the literature. Oncol Lett. 2014 Oct;8(4):1825-1827. doi: 10.3892/ol.2014.2326. Epub 2014 Jul 8. PMID: 25202418; PMCID: PMC4156199.
- Ali AM, Mirrakhimov AE, Abboud CN, Cashen AF. Leukostasis in adult acute hyperleukocytic leukemia: a clinician's digest. Hematol Oncol. 2016 Jun;34(2):69-78. doi: 10.1002/hon.2292. Epub 2016 Mar 27. PMID: 27018197.
- Giammarco S, Chiusolo P, Piccirillo N, Di Giovanni A, Metafuni E, Laurenti L, Sica S, Pagano L. Hyperleukocytosis and leukostasis: management of a medical emergency. Expert Rev Hematol. 2017 Feb;10(2):147-154. doi: 10.1080/17474086.2017.1270754. Epub 2016 Dec 26. PMID: 27967252.
- Kong SG, Seo JH, Jun SE, Lee BK, Lim YT. Childhood acute lymphoblastic leukemia with hyperleukocytosis at presentation. Blood Res. 2014 Mar;49(1):29-35. doi: 10.5045/br.2014.49.1.29. Epub 2014 Mar 24. PMID: 24724064; PMCID: PMC3974953.
- Farhan S, Anjum F, Al-Qahtani FS and Al-Anazi KA. Chronic myeloid leukemia presenting with priapism. J Leuk 2015; 3:171. doi: 10.4172/23296917.1000171
- Kittivisuit S, Jongthitinon N, Sripornsawan P, Songthawee N, Chavananon S, Limratchapong C, McNeil EB, Chotsampancharoen T. Hyperleukocytosis in Childhood Acute Leukemia: Early Complications and Survival Outcomes. Cancers (Basel). 2023 Jun 6;15(12):3072. doi: 10.3390/cancers15123072. PMID: 37370683; PMCID: PMC10295972.
- Bewersdorf JP, Zeidan AM. Hyperleukocytosis and Leukostasis in Acute Myeloid Leukemia: Can a Better Understanding of the Underlying Molecular Pathophysiology Lead to Novel Treatments? Cells. 2020 Oct 17;9(10):2310. doi: 10.3390/cells9102310. PMID: 33080779; PMCID: PMC7603052.
- Aqui N, O'Doherty U. Leukocytapheresis for the treatment of hyperleukocytosis secondary to acute leukemia. Hematology Am Soc Hematol Educ Program. 2014 Dec 5;2014(1):457-60. doi: 10.1182/asheducation-2014.1.457. Epub 2014 Nov 18. PMID: 25696894.
- Aswanetmanee P, Edriss H, Limsuwat C. Pulmonary leukostasis as a complication of leukemia. Southwest Respir Crit Care Chron. 2015; 3(10): 17-22. doi: 10.12746/swrccc2015.0310.028
- Singh H, Prasad BN, Jagdish, Batra A. Hyperleukocytosis associated pulmonary leukostasis in acute leukaemia. J Assoc Physicians India. 2006 May;54:405-7. PMID: 16909741.
- Rico-Rodríguez J, Villanueva-Ortiz Á, Santana-Cabrera L, Rodríguez-Pérez H. Pulmonary leukostasis with severe respiratory impairment as a debut of acute myeloid leukemia. Int J Crit Illn Inj Sci. 2015 Apr-Jun;5(2):125-6. doi: 10.4103/2229-5151.158423. PMID: 26157660; PMCID: PMC4477392.
- Zhang D, Lin H, Huang L. Repeated small-volume exchange transfusion for hyperleukocytosis in pediatric acute leukemia: A retrospective analysis. Front Pediatr. 2023 Mar 22;11:1155481. doi: 10.3389/fped.2023.1155481. PMID: 37033185; PMCID: PMC10073680.
- Haase R, Merkel N, Diwan O, Elsner K, Kramm CM. Leukapheresis and exchange transfusion in children with acute leukemia and hyperleukocytosis. A single center experience. Klin Padiatr. 2009 Nov-Dec;221(6):374-8. doi: 10.1055/s-0029-1239533. Epub 2009 Nov 4. PMID: 19890790.
- Zhang D, Zhu Y, Jin Y, Kaweme NM, Dong Y. Leukapheresis and Hyperleukocytosis, Past and Future. Int J Gen Med. 2021 Jul 14;14:3457-3467. doi: 10.2147/IJGM.S321787. PMID: 34285568; PMCID: PMC8286901.
- Thapa N, Pham R, Cole C, Meinershagen M, Bowman PW, Ray A. Therapeutic leukocytapheresis in infants and children with leukemia and hyperleukocytosis: A single institution experience. J Clin Apher. 2018 Jun;33(3):316-323. doi: 10.1002/jca.21610. Epub 2017 Nov 29. PMID: 29193219.
- Bruserud Ø, Liseth K, Stamnesfet S, Cacic DL, Melve G, Kristoffersen E, Hervig T, Reikvam H. Hyperleukocytosis and leukocytapheresis in acute leukaemias: experience from a single centre and review of the literature of leukocytapheresis in acute myeloid leukaemia. Transfus Med. 2013 Dec;23(6):397-406. doi: 10.1111/tme.12067. Epub 2013 Aug 6. PMID: 23919332.
- Choi MH, Choe YH, Park Y, Nah H, Kim S, Jeong SH, Kim HO. The effect of therapeutic leukapheresis on early complications and outcomes in patients with acute leukemia and hyperleukocytosis: a propensity score-matched study. Transfusion. 2018 Jan;58(1):208-216. doi: 10.1111/trf.14329. Epub 2017 Sep 28. PMID: 28960357.
- Pastore F, Pastore A, Wittmann G, Hiddemann W, Spiekermann K. The role of therapeutic leukapheresis in hyperleukocytotic AML. PLoS One. 2014 Apr 14;9(4):e95062. doi: 10.1371/journal.pone.0095062. PMID: 24733550; PMCID: PMC3986260.
- Malkan UY, Ozcebe OI. Leukapheresis do not improve early death rates in acute myeloid leukemia patients with hyperleukocytosis. Transfus Apher Sci. 2017 Dec;56(6):880-882. doi: 10.1016/j.transci.2017.11.002. Epub 2017 Nov 8. PMID: 29153308.
- Rinaldi I, Sari RM, Tedhy VU, Winston K. Leukapheresis Does Not Improve Early Survival Outcome of Acute Myeloid Leukemia with Leukostasis Patients - A Dual-Center Retrospective Cohort Study. J Blood Med. 2021 Jul 14;12:623-633. doi: 10.2147/JBM.S312140. PMID: 34290537; PMCID: PMC8286962.
- Oberoi S, Lehrnbecher T, Phillips B, Hitzler J, Ethier MC, Beyene J, Sung L. Leukapheresis and low-dose chemotherapy do not reduce early mortality in acute myeloid leukemia hyperleukocytosis: a systematic review and meta-analysis. Leuk Res. 2014 Apr;38(4):460-8. doi: 10.1016/j.leukres.2014.01.004. Epub 2014 Jan 10. PMID: 24472688.
- Göçer M, Kurtoğlu E. Effect of prophylactic leukapheresis on early mortality and overall survival in acute leukemia patients with hyperleukocytosis. Ther Apher Dial. 2021 Oct;25(5):697-703. doi: 10.1111/1744-9987.13645. Epub 2021 Apr 7. PMID: 33686785.
- Berber I, Kuku I, Erkurt MA, Kaya E, Bag HG, Nizam I, Koroglu M, Ozgul M, Bazna S. Leukapheresis in acute myeloid leukemia patients with hyperleukocytosis: A single center experience. Transfus Apher Sci. 2015 Oct;53(2):185-90. doi: 10.1016/j.transci.2015.03.015. Epub 2015 Mar 18. PMID: 25843763.
- Bug G, Anargyrou K, Tonn T, Bialleck H, Seifried E, Hoelzer D, Ottmann OG. Impact of leukapheresis on early death rate in adult acute myeloid leukemia presenting with hyperleukocytosis. Transfusion. 2007 Oct;47(10):1843-50. doi: 10.1111/j.1537-2995.2007.01406.x. PMID: 17880610.
- Nan X, Qin Q, Gentille C, Ensor J, Leveque C, Pingali SR, Phan AT, Rice L, Iyer S. Leukapheresis reduces 4-week mortality in acute myeloid leukemia patients with hyperleukocytosis - a retrospective study from a tertiary center. Leuk Lymphoma. 2017; 58(9): 1-11. doi: 10.1080/10428194.2016.1277386. Epub 2017 Jan 31.
- Lee H, Park S, Yoon JH, Cho BS, Kim HJ, Lee S, Kim DW, Chung NG, Cho B, Kim KB, Yoo J, Jekarl DW, Chae H, Lim J, Kim M, Oh EJ, Kim Y. The factors influencing clinical outcomes after leukapheresis in acute leukaemia. Sci Rep. 2021 Mar 19;11(1):6426. doi: 10.1038/s41598-021-85918-8. PMID: 33742034; PMCID: PMC7979875.
- Aragona M, Aragona F. Morte inattesa da leucostasi e da tumori leucostatici polmonari nelle leucemie mieloidi acute. Studio su quattro casi [Unexpected death by leukostasis and lung leukostatic tumors in acute myeloid leukemia. Study of four cases]. Minerva Med. 2000 Oct;91(10):229-37. Italian. PMID: 11236388.
- Creutzig U, Ritter J, Budde M, Sutor A, Schellong G. Early deaths due to hemorrhage and leukostasis in childhood acute myelogenous leukemia. Associations with hyperleukocytosis and acute monocytic leukemia. Cancer. 1987 Dec 15;60(12):3071-9. doi: 10.1002/1097-0142(19871215)60:12<3071::aid-cncr2820601235>3.0.co;2-y. PMID: 3479232.
- Pryds K, Rasmussen LE, Andersen NH. Fatal right-sided heart failure due to leukostasis in a patient with leukemic transformation of myelodysplastic syndrome. Clin Case Rep. 2018 Nov 20;7(1):115-119. doi: 10.1002/ccr3.1929. PMID: 30656022; PMCID: PMC6332819.
- Katogiannis K, Ikonomidis I, Panou F, Katsimardos A, Divane A, Tsantes A, Iliodromitis E, Kyriakou E. Leukostasis-related fatal cardiopulmonary arrest as initial chronic myeloid leukemia presentation. J Med Cases. 2018; 9(3): 77-82. doi: https://doi.org/10.14740/ jmc2993w
- Day M, Jalli S, Harkness W, Earley T. Leukostasis from CML leading to sudden cardiac death. J Am Coll Cardiol. 2022, 79 (9_Supplement) 2995.doi: 10.1016/S0735-1097(22)03986-9
- Takahashi N, Sano H, Mochizuki K, Kobayashi S, Ohara Y, Kikuta A. Intracranial Hemorrhage in a Pediatric Patient with Chronic Myeloid Leukemia in Chronic Phase: A Case Report. Case Rep Oncol. 2021 Mar 22;14(1):525-530. doi: 10.1159/000515011. PMID: 33976629; PMCID: PMC8077513.
- Ashraf M, Naseeruddin G, Zahra SG, Sultan KA, Kamboh UA, Manzoor M, Farooq M, Ahmad M, Ashraf N. Intracerebral hemorrhage as the first symptomatic manifestation of chronic myeloid leukemia (chronic phase): A case report and literature review. Surg Neurol Int. 2023 Jan 6;14:5. doi: 10.25259/SNI_897_2022. PMID: 36751457; PMCID: PMC9899481.
- Tien FM, Hou HA, Tsai CH, Tang JL, Chen CY, Kuo YY, Li CC, Lin CT, Yao M, Huang SY, Ko BS, Hsu SC, Wu SJ, Tsay W, Tseng MH, Liu MC, Liu CW, Lin LI, Chou WC, Tien HF. Hyperleukocytosis is associated with distinct genetic alterations and is an independent poor-risk factor in de novo acute myeloid leukemia patients. Eur J Haematol. 2018 Jul;101(1):86-94. doi: 10.1111/ejh.13073. Epub 2018 May 22. PMID: 29624746.
- Canaani J, Labopin M, Socié G, Nihtinen A, Huynh A, Cornelissen J, Deconinck E, Gedde-Dahl T, Forcade E, Chevallier P, Bourhis JH, Blaise D, Mohty M, Nagler A. Long term impact of hyperleukocytosis in newly diagnosed acute myeloid leukemia patients undergoing allogeneic stem cell transplantation: An analysis from the acute leukemia working party of the EBMT. Am J Hematol. 2017 Jul;92(7):653-659. doi: 10.1002/ajh.24737. Epub 2017 May 26. PMID: 28370339.
- Feng S, Zhou L, Zhang X, Tang B, Zhu X, Liu H, Sun Z, Zheng C. Impact Of ELN Risk Stratification, Induction Chemotherapy Regimens And Hematopoietic Stem Cell Transplantation On Outcomes In Hyperleukocytic Acute Myeloid Leukemia With Initial White Blood Cell Count More Than 100 × 109/L. Cancer Manag Res. 2019 Nov 8;11:9495-9503. doi: 10.2147/CMAR.S225123. PMID: 31807075; PMCID: PMC6850690.