
More Information
Submitted: May 25, 2026 | Accepted: June 05, 2026 | Published: June 08, 2026
Citation: Patel S, Hirani D. Myeloma Presenting with Paraneoplastic Syndrome: Inflammatory-demyelinating Condition of the Central Nervous System. J Hematol Clin Res. 2026; 10(1): 31-33. Available from:
https://dx.doi.org/10.29328/journal.jhcr.1001042
DOI: 10.29328/journal.jhcr.1001042
Copyright license: © 2026 Patel S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Myeloma Presenting with Paraneoplastic Syndrome: Inflammatory-demyelinating Condition of the Central Nervous System
Sneha Patel* and Dhillon Hirani
and Dhillon Hirani
Luton and Dunstable University Hospital NHS Foundation Trust: Luton, England
*Corresponding author: Dr. Sneha Patel, Luton and Dunstable University Hospital NHS Foundation Trust: Luton, England, Email: [email protected]
Multiple myeloma (MM) is a clonal plasma cell malignancy classically presenting with CRAB features: hypercalcaemia, renal impairment, anaemia and osteolytic bone disease. Paraneoplastic neurological manifestations are rare and poorly characterised, with evidence limited largely to isolated case reports. We describe an unusual case of MM presenting with recurrent inflammatory-demyelinating central nervous system (CNS) disease, demonstrating diagnostic complexity and responsiveness to anti-myeloma therapy.
Multiple Myeloma (MM) is a clonal plasma cell disorder characterised by overproduction of monoclonal immunoglobulins leading to end-organ damage. It most commonly presents with CRAB features — hypercalcaemia, renal impairment, anaemia and osteolytic lesions [1].
Paraneoplastic manifestations of MM are rare, with evidence largely limited to isolated case reports [2]. Reported paraneoplastic manifestations of MM include Sweet syndrome, sarcoidosis, polycythaemia, myasthenia gravis, Guillain–Barré syndrome, and other dermatological conditions [3]. Neurological paraneoplastic presentations are particularly uncommon. Reported cases include acute disseminated encephalomyelitis, CIDP and multifocal neurological deficits, with documented responses to combined corticosteroid and chemotherapy [4,5].
Here, we report a case of MM presenting with an inflammatory-demyelinating condition of the central nervous system, highlighting diagnostic difficulties and expanding the recognised spectrum of paraneoplastic presentations.
A 54-year-old male presented to the Emergency Department with bilateral blurred vision three weeks following a viral respiratory infection. He was clinically diagnosed with optic neuritis and treated with IV Methylprednisolone, which moderately improved his symptoms. MRI imaging showed nonspecific focal areas of T2 hyperintensities with no space-occupying lesions or signs of demyelination in his spine. In his CSF, the cell count was: 0 white blood cells and 0 red blood cells. The appearance was a clear, colourless fluid. The biochemistry of the CSF was also obtained, and it had normal glucose at 3.7 mmol/L (normal range between 2.2 – 3.9 mmol/L). The total protein level was slightly increased at 0.59 g/L (normal range between 0.15 – 0.45 g/L). CSF oligoclonal bands were requested, and the results showed monoclonal bands in the CSF. In the serum, the oligoclonal bands were not investigated.
He was readmitted two months later with dysphasia, which again was treated with steroids, resulting in resolution of his symptoms. A repeat MRI showed a new focus of high signal on flair imaging, again suggestive of an underlying inflammatory/demyelinating process (images included)(Images 1-3).
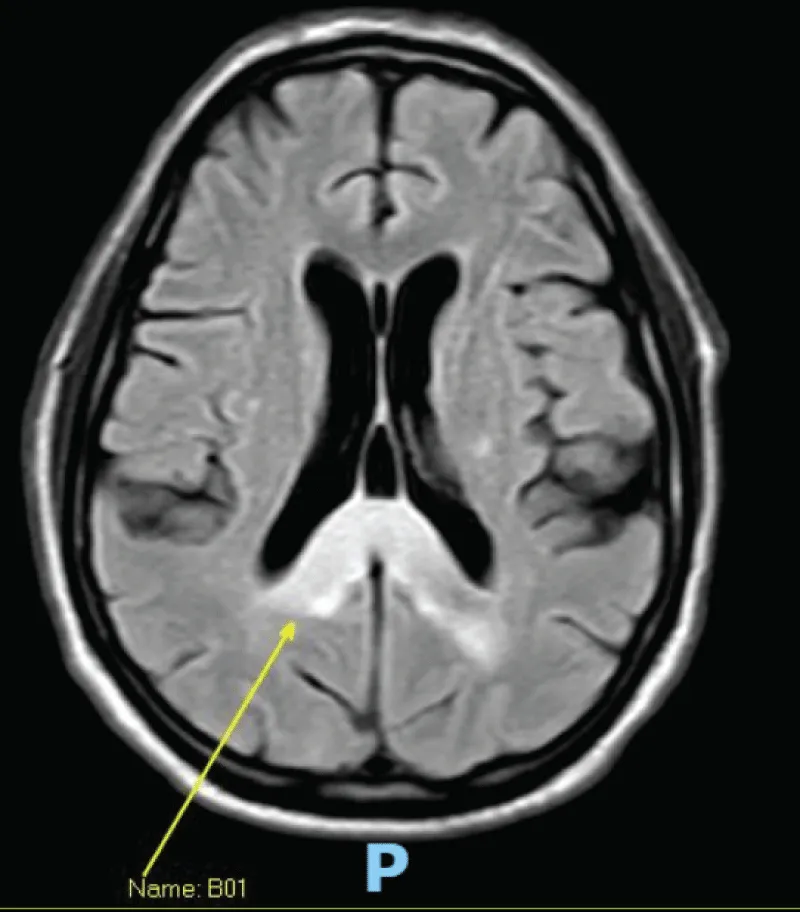
Image 1: MRI image.
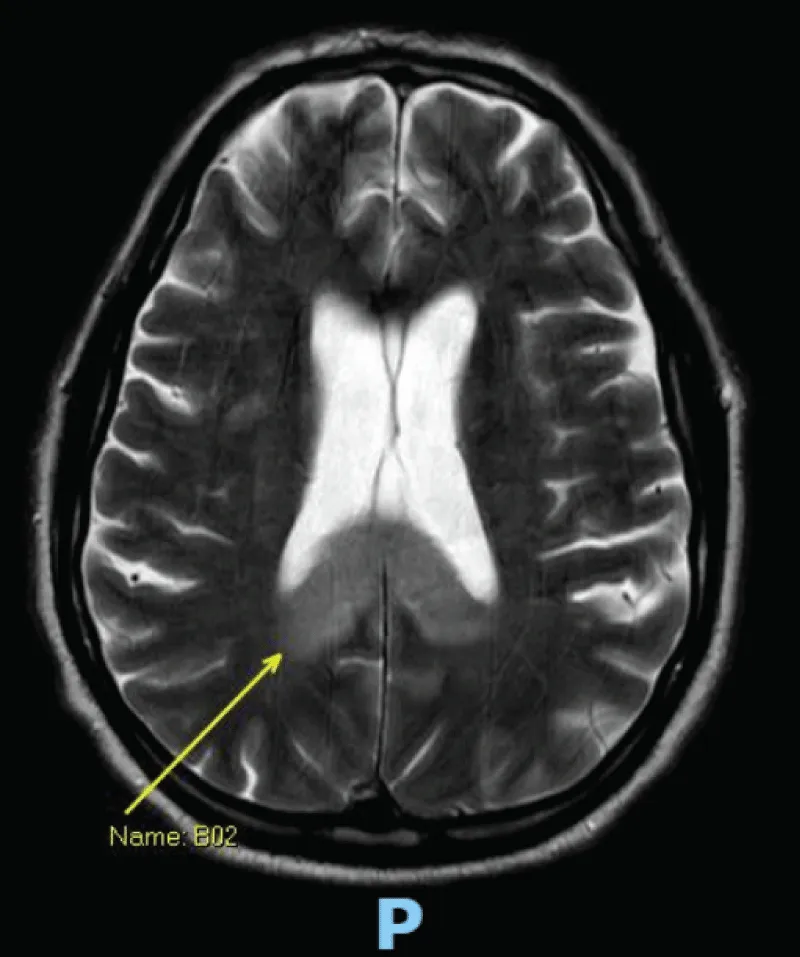
Image 2: MRI image.
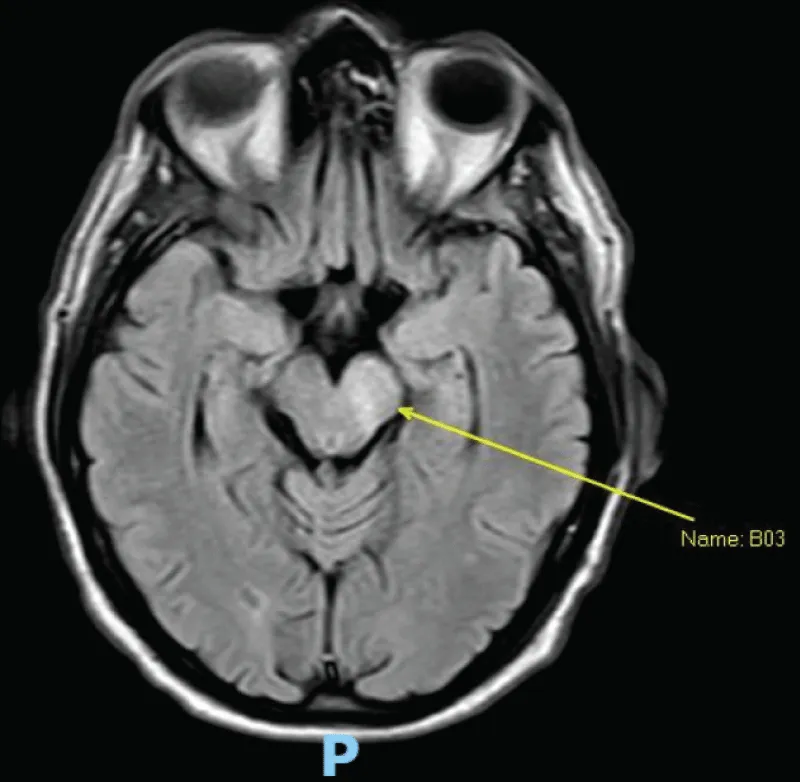
Image 3: MRI image.
He was readmitted a month later with bilateral pulmonary embolism (PE). Considering the diagnosis of PE and his previous LP showing the presence of monoclonal bands, he was investigated for a possible neoplasm. His blood tests showed IgG Lambda paraproteinaemia of 2 g/L, Kappa light chains 8.3 mg/L, Lambda light chains 115.3 mg/L (Kappa Lambda ratio 0.01), and the bone marrow biopsy revealed 20% plasma cells with FISH showing gain of 5p, 9q and 15q (standard risk) consistent with a diagnosis of myeloma. A whole-body CT scan showed multiple lytic bone lesions.
Within four months, he had gone from being asymptomatic and physically active to having dysarthria, limb paraesthesia, impaired coordination, and difficulty walking. An MDT approach with neurology concluded that he suffered from an inflammatory-demyelinating condition of the central nervous system, which may be related to the presence of a neoplastic condition, such as myeloma.
He was started on Velcade, Cyclophosphamide, and Dexamethasone (VCD). Following four cycles of chemotherapy, he dramatically improved both symptomatically and biochemically. His paraprotein was unquantifiable, and lambda light chains went down to 20 mg/L. He was able to walk several miles a day with significant improvement in his neuropathy. Unfortunately, his eyesight did not improve but reassuringly remained stable.
He had a Melphalan autologous stem cell transplant and then continued maintenance lenalidomide. He remained stable for about four years on lenalidomide. However, 5 years on from his initial presentation, he presented to the Emergency Department with right-sided numbness, weakness, slurred speech, facial droop, and expressive aphasia worsening over a few days. He was initially managed as having a left MCA infarct with the MRI head showing a posterior limb of the internal capsule (PLIC) signal compatible with an acute infarct, but also a signal crossing the corpus callosum that was not typical for this. Differentials included malignancy, demyelination, and infection.
The MDT requested a biopsy of the corpus callosum. The biopsies showed no evidence of neoplasm, Progressive Multifocal Leukoencephalopathy, demyelination, or granulomatous disease, and showed prominent macrophages that were thought to likely represent phagocytic debris. Fungal disease was excluded. CSF did not show any evidence of haematological malignancy and was negative for virology, including JC virus.
During this hospital stay, he continued to deteriorate and he became unable to communicate verbally or move any of his limbs. His GCS progressively declined therefore needing intubation. His neurology at the time showed a mixed upper and low motor neuron picture with hyperreflexia, upgoing plantar reflexes but global hypotonia. It was hypothesised that these symptoms could again represent paraneoplastic phenomenon.
Biochemically his blood tests showed kappa light chains of 8.36 mg/L and a slight increase in lambda free light chains of 108 mg/L resulting in a ratio of 0.08. Considering his rapid deterioration he was discussed at the Haematology MDT meeting which agreed to start chemotherapy in attempt to salvage his condition. This was agreed with the patient’s family.
The patient started second-line treatment with Daratumumab, Velcade and Dexamethasone (DVD). A couple of weeks later, his GCS improved and he was extubated. Repeat MRIs showed stable changes. Following the first cycle, kappa light chains improved to 3.96 mg/L, lambda light chains were 20.7 mg/L with a ratio of 0.19.
The patient continued to improve on chemotherapy. After rehabilitation, he is now able to maintain a good conversation and has better strength.
Paraneoplastic manifestations of MM are rare, with evidence largely limited to isolated case reports and have not been considered in any formal guidelines. Other more recognised CNS involvement, although uncommon include dural plasmacytomas, parenchymal brain lesions or spinal involvement with epidural plasmacytomas causing spinal cord compression where the recommended treatment is radiotherapy. These would be evident on imaging. Leptomeningeal involvement would present with plasma cell infiltrate in the CSF. This case expands on the spectrum of neurological paraneoplastic phenomena associated with MM and highlights the importance of considering plasma cell dyscrasia in unexplained inflammatory-demyelinating CNS disease. The correlation between neurological deterioration and myeloma activity, together with repeated clinical responses to anti-myeloma therapy, supports a likely paraneoplastic mechanism.
- Albagoush SA, Shumway C, Azevedo AM. Multiple Myeloma. StatPearls. Treasure Island: StatPearls Publishing; 2026. Available from: https://pubmed.ncbi.nlm.nih.gov/30521185/
- Baloch SS, Khan SR, Tariq M, Wasio A, Ali AA, Shahzadi, M, et al. Multiple myeloma and its rare paraneoplastic manifestations simmering under the surface. Pathology - Research and Practice, 2023; 248:154689. Available from: https://doi.org/10.1016/j.prp.2023.154689
- Smith N, Kimberger K, Parrish C, Currie S, Butterworth S, Alty J. Multiple myeloma with multiple neurological presentations. Practical Neurology, 2019; 19(6): 511–517.
- Law LY and Nagao KJ. Paraneoplastic acute disseminated encephalomyelitis associated with multiple myeloma. Multiple Sclerosis and Related Disorders, 2017;13: 21–24. Available from: https://doi.org/10.1016/j.msard.2017.01.013
- Fasanya AA, Loncharich MF, Gandhi V, Rana S, Balaan M. Multiple Myeloma Associated Chronic Inflammatory Demyelinating Polyradiculoneuropathy: The Importance of Continued Surveillance. Cureus, 2016;8(11): 899. Available from: https://doi.org/10.7759/cureus.899